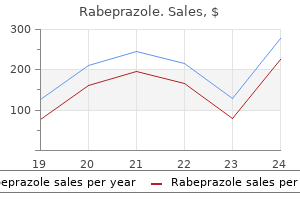
Only $0.48 per item
Rabeprazole dosages: 20 mg, 10 mg
Rabeprazole packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 983
10 of 10
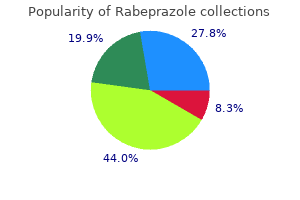
Votes: 72 votes
Total customer reviews: 72
Description
Decreasing mortality from acute biliary diseases that require endoscopic retrograde cholangiopancreatogra phy: a nationwide cohort study gastritis empty stomach discount rabeprazole 10 mg buy line. Delayed endoscopic retrograde cholangiopancreatog raphy is associated with persistent organ failure in hospital ised patients with acute cholangitis. The remainder of cases are caused by blunt external injury to the abdomen, pancreatitis, erosion of the duct by a gallstone, or prior endoscopic sphincterotomy. Signs of injury to the duct may or may not be recog nized in the immediate postoperative period. If complete occlusion has occurred, j aundice will develop rapidly; more often, however, a tear has been made accidentally in the duct, and the earliest manifestation of injury may be excessive or prolonged loss of bile from the surgical drains. Bile leakage resulting in a bile collection (biloma) may predispose to localized infection, which in turn accentuates scar formation and the ultimate development of a fibrous stricture. Typically, the patient experiences episodes of pain, fever, chills, and j aundice within a few weeks to months after cholecystectomy. Physical findings may include j aun dice during an acute attack of cholangitis and right upper quadrant abdominal tenderness. Hyperbilirubinemia is variable, fluctuating during exacerbations and usually remaining in the range of 5 - 1 0 mg/dL (85. Secondary biliary cirrhosis will inevitably develop if a stricture is not treated. Placement of multiple plastic stents appears to be more effective than placement of a single stent. The use of covered metal stents, which are more easily removed endo scopically than uncovered metal stents, as well as bioab sorbable stents, is an alternative to use of plastic stents. Uncovered metal stents, which often cannot be removed endoscopically, are generally avoided in benign strictures unless life expectancy is less than 2 years. Strictures related to chronic pancreatitis are more difficult than postsurgical strictures to treat endoscopically and may be best managed with a temporary covered metal stent. Following liver transplantation, endoscopic management is more success ful for anastomotic than for nonanastomotic strictures, although results for nonanastomotic strictures may be improved with repeated dilation or the use of multiple plas tic stents. Differentiation from cholangiocarcinoma may ultimately require surgical explo ration. Operative treatment of a stricture frequently neces sitates performance of an end-to-end ductal repair, choledochojejunostomy, or hepaticojejunostomy to rees tablish bile flow into the intestine. Successful management of benign biliary strictures with fully covered self- expanding metal stents. Single-operator cholangioscopy and targeted biopsies in the diagnosis of indeterminate biliary strictures: a systematic review. General Considerations Primary sclerosing cholangitis is an uncommon disease thought to result from an increased immune response to intestinal endotoxins and characterized by diffuse inflam mation of the biliary tract leading to fibrosis and strictures of the biliary system.
Wordward (Sweet Woodruff). Rabeprazole.
- What is Sweet Woodruff?
- Dosing considerations for Sweet Woodruff.
- How does Sweet Woodruff work?
- Preventing and treating lung, stomach, liver, gallbladder, and urinary disorders; nervousness; hemorrhoids; sleeplessness; migraines; skin problems; and other conditions.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96113
About two-thirds of the preterm births occur between 34 weeks and 36 weeks and 6 days (termed late preterm birth) gastritis length generic rabeprazole 10 mg without a prescription, and good outcomes are expected at these gestational ages. Importantly, however, even these late preterm infants are at significantly increased risk for both morbidity and mortality when compared to those infants born at term. Maj or risk factors for spontaneous preterm labor include a past history of preterm birth and a short cervi cal length as measured by transvaginal ultrasound. Patients with one or both of these risk factors have largely been the focus of recent intervention trials aiming to prevent pre term birth. Other known risk factors are many but include black race, multi-fetal pregnancies, intrauterine infection, substance abuse, smoking, periodontal disease, and socio economic deprivation. Corticosteroids In pregnancies between 24 and 34 weeks gestation where preterm birth is anticipated, a single short course of corti costeroids should be administered to promote fetal lung maturity. Such therapy has been demonstrated to reduce the frequency of respiratory distress syndrome, intracra nial hemorrhage, and even death in preterm infants. Beta methasone, 12 mg intramuscularly repeated once 24 hours later, or dexamethasone, 6 mg intramuscularly repeated every 12 hours for four doses, both cross the placenta and are the preferred treatments in this setting. Although antibiotics have not been proven to forestall delivery, women in preterm labor should receive antimicrobial prophylaxis against group B streptococcus. Tocolytic Agents Numerous pharmacologic agents-tocolytics-have been given in an attempt to forestall preterm birth, although none are completely effective, and there is no evidence that such therapy directly improves neonatal outcomes. Maintenance therapy (continuation of treatment beyond 48 hours) is not effective at preventing preterm birth and is not recommended. Likewise, despite the finding that preterm labor is associated with intrauter ine infection in certain cases, there is no evidence that antibiotics forestall delivery in women with preterm labor and intact membranes. Magnesium sulfate is commonly used, and there is evidence that it may also be protective against cerebral palsy in infants whose mothers were receiving magnesium infusions at time of birth. Magnesium sulfate is given intra venously as a 4- to 6-g bolus followed by a continuous infusion of 2 g/h. Magnesium levels are not typically checked but should be monitored if there is any concern for toxicity. Magnesium sulfate is entirely cleared by the kidney and must, therefore, be used with caution in women with any degree of kidney disease. B eta- adrenergic drugs such as terbutaline can be given as an intravenous infusion starting at 2. Oral terbutaline is not recommended because of the lack of proven efficacy and concerns about maternal safety. Serious maternal side effects have been reported with the use of terbutaline and include tachycardia, pulmo nary edema, arrhythmias, metabolic derangements (such as hyperglycemia and hypokalemia), and even death. Pul monary edema occurs with increased frequency with con comitant administration of corticosteroids, large volume intravenous fluid infusion, maternal sepsis, or prolonged tocolysis.
Specifications/Details
Reported extrahepatic manifestations include arthritis; pancreatitis; monoclonal gammopathy; thrombocytope nia; and a variety of neurologic complications gastritis diet ������� rabeprazole 10 mg order fast delivery, including Guillain-Barre syndrome and peripheral neuropathy. The risk of hepatic decompensation is increased in patients with underlying chronic liver disease. Nosocomial hepatitis C virus transmission from tampering with injectable anesthetic opioids. The overall mortality rate is less than 1 %, but the rate is reportedly higher in older people. Chronic hepatitis, which progresses very slowly in many cases, develops in as many as 85% of all persons with acute hepatitis C. Patients with cir rhosis are at risk for hepatocellular carcinoma at a rate of 3-5% per year. Ful minant hepatic failure is characterized by the development of hepatic encephalopathy within 8 weeks after the onset of acute liver disease. Subfulmi nant hepatic failure occurs when these findings appear between 8 weeks and 6 months after the onset of acute liver disease and carries an equally poor prognosis. Acute-on chronic liver failure refers to acute deterioration in liver function in a person with preexisting chronic liver disease. An estimated 1 600 cases of acute liver failure occur each year in the United States. Acetaminophen toxicity is the most common cause, accounting for at least 45% of cases. Suicide attempts account for 44% of cases of acet aminophen-induced hepatic failure, and unintentional overdoses ("therapeutic misadventures"), which are often a result of a decrease in the threshold toxic dose because of chronic alcohol use or fasting and have been reported after weight loss surgery, account for at least 48%. Other causes include idiosyncratic drug reactions (the second most common cause, with antituberculosis drugs, antiepileptics, and antibiotics implicated most commonly), viral hepatitis, poisonous mushrooms (Amanita phalloides), shock, hyper thermia or hypothermia, Budd-Chiari syndrome, malig nancy (most commonly lymphomas), Wilson disease, Reye syndrome, fatty liver of pregnancy and other disorders of fatty acid oxidation, autoimmune hepatitis, parvovirus B 1 9 infection and, rarely, grand mal seizures. Herbal and dietary supplements are thought to be contributory to acute liver failure in a substantial portion of cases, regardless of cause. Acute-on-chronic liver failure is often precipitated by infection or an alcohol binge and alcoholic hepatitis. The decline of viral hepatitis as the prin cipal cause of acute liver failure is due to universal vaccina tion of infants and children against hepatitis B and the availability of the hepatitis A vaccine. Hepatitis C is a rare cause of acute liver failure in the United States, but acute hepatitis A or B superimposed on chronic hepatitis C may cause fulminant hepatitis. Adrenal insufficiency and subclinical myocardial injury manifesting as an elevated serum troponin I level often complicate acute liver failure. Jaundice may be absent or minimal early, but laboratory tests show severe hepatocellular damage. In acetaminophen toxicity, serum aminotransferase elevations are often towering (greater than 5000 units/L). In acute liver failure due to microvesicular steatosis (eg, fatty liver of pregnancy), serum aminotransferase elevations may be modest (less than 300 units/L). Over 10% of patients have an elevated serum amylase level at least three times the upper limit of normal, often as a result of renal dysfunction.
Syndromes
- Low reticulocyte count (reticulocytes are immature red blood cell)
- Infections of the skin caused by bacteria, fungi, or viruses
- Serum magnesium
- Bend forward, backward, and sideways
- Heart failure
- Magnetic resonance imaging (MRI) of the heart, which provides a detailed image of the heart through the use of powerful magnets
- Fluorides
- Long-term avoidance of feelings
- If the medication was prescribed for the patient
- Hepatitis B and C antibodies
Such thyrotoxic crisis can be precipi tated by trauma gastritis joint pain 20 mg rabeprazole purchase overnight delivery, infection, surgery, or delivery and confers a fetal/maternal mortality rate of about 25%. Such thyrotoxic newborns have an increased risk of intrauterine growth retardation and prematurity. It usually presents abruptly with symmetric flaccid paralysis (and few thyrotoxic symptoms), often after intravenous dextrose, oral carbohydrate, or vigorous exercise. Serum T3 can be misleadingly elevated when blood is col lected in tubes using a gel barrier, which causes certain immunoassays to report falsely elevated serum total T 3 levels in 24% of normal patients. Hyperthyroidism can cause other laboratory abnor malities, including hypercalcemia, increased alkaline phos phatase, anemia, and decreased granulocytes. Problems of diagnosis occur in patients with acute psy chiatric disorders; about 30% of these patients have ele vated serum T4 levels without clinical thyrotoxicosis. Antithyroglobulin or antithyroperoxidase antibod ies are usually elevated but are nonspecific. In thyrotoxicosis factitia, serum thyroglobulin levels are low, distinguishing it from other causes of hyperthyroidism. Although the serum T4 is elevated in most pregnant women, values over 20 mcg/dL (257 nmoi! Technetium (Tc- 99m) pertechnetate is given intrave nously, and scanning is performed 20 minutes later. Technetium (Tc- 99m) pertechnetate mimics radioiodine scanning but is more convenient, costs less, and confers less radiation exposure. Thyroid ultrasound can be helpful in patients with hyperthyroidism, particularly in patients with palpable thyroid nodules. Thyroid ultrasound shows a variably het erogenous, hypoechoic gland in thyroiditis. Color flow Doppler sonography is helpful to distinguish type 1 amio darone-induced thyrotoxicosis (normal to increased blood flow velocity and vascularity) from type 2 amiodarone induced thyrotoxicosis (reduced vascularity). Imaging is required only in severe or unilateral cases or in euthyroid exophthalmos that must be distinguished from orbital pseudotumor, tumors, and other lesions. Some states of hypermetabolism without thyrotoxico sis-notably severe anemia, leukemia, polycythemia, can cer, and pheochromocytoma-rarely cause confusion. Ocular myasthenia gravis is another autoimmune condi tion that occurs more commonly in Graves disease but is usually mild, often with unilateral eye involvement. Complications Hypercalcemia, osteoporosis, and nephrocalcinosis may occur in hyperthyroidism. Decreased libido, erectile dysfunc tion, diminished sperm motility, and gynecomastia may be noted in men. Other complications include cardiac arrhyth mias and heart failure, thyroid crisis, ophthalmopathy, der mopathy, and thyrotoxic hypokalemic periodic paralysis.
Related Products
Additional information:
Usage: q.d.
Tags: generic rabeprazole 10 mg otc, cheap rabeprazole 20 mg on-line, rabeprazole 10 mg fast delivery, buy rabeprazole 10 mg without a prescription
Customer Reviews
Real Experiences: Customer Reviews on Aciphex
Gorok, 29 years: Emptying of the gallbladder may be markedly reduced on gallbladder scintigraphy fol lowing injection of cholecystokinin; cholecystectomy may be curative in such cases.
Sugut, 62 years: Definitive surgery depends on the degree of disability and the findings at operation.
Hurit, 59 years: The mortality rate due to the underlying disease is high (particularly in patients receiving vasopressor therapy or with septic shock, acute kidney disease, or coagu lopathy), but in patients who recover, the aminotransferase levels return to normal quickly, usually within 1 week-in contrast to viral hepatitis.
Grim, 44 years: Fungal infection with mucormycosis and Candida may occur in immunocompromised and diabetic patients.
Karlen, 24 years: Intravenous antibiotics should be continued for 5-7 days, before changing to oral antibiotics.
Redge, 49 years: Gynecologic procedures: colposcopy, treatments for cervical intraepithelial neoplasia and endometrial assess ment.
Asam, 23 years: This diar rhea commonly responds to cholestyramine 2-4 g, colesti pol 5 g, or colesevelam 625 mg one to two times daily before meals to bind the malabsorbed bile salts.