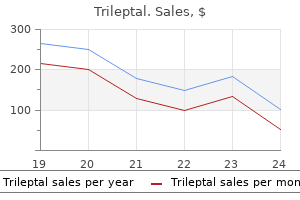
Only $0.56 per item
Trileptal dosages: 600 mg, 300 mg, 150 mg
Trileptal packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 582
10 of 10
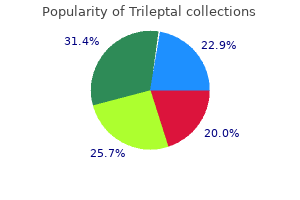
Votes: 112 votes
Total customer reviews: 112
Description
Treatment is problematic treatment jones fracture order trileptal 150 mg, although some success has been reported with phosphate-binding antacids, calcium deprivation, calcitonin, and acetazolamide therapy. Most cases of hyperphosphatemia associated with intestinal phosphate loads have involved children who received phosphate-containing laxatives or enemas or older adults with impaired renal function receiving phosphate-based cathartics in preparation for colonoscopy. This disorder was described initially as a complication of rapid induction chemotherapy for certain hematologic malignancies (tumor lysis syndrome), although it also may occur from cellular injury associated with trauma, hyperthermia, overwhelming infection, hemolysis, rhabdomyolysis, or metabolic acidosis. The clinical manifestations of acute, severe hyperphosphatemia are related mainly to those of the accompanying hypocalcemia, caused by formation of insoluble calcium phosphate precipitates. Thus, tetany, muscle cramps, paresthesias, and seizures may occur, and they may be compounded by other metabolic disturbances (hyperkalemia, acidosis, hyperuricemia) that frequently coexist. Generalized precipitation of calcium phosphate into soft tissues may produce organ dysfunction, notably renal failure. Identification and removal of any exogenous sources of phosphate are important, and phosphatebinding aluminum hydroxide antacids may be useful in limiting intestinal phosphate absorption and chelating phosphate secreted into the intestine. Hemodialysis is the most effective approach and should be considered early in severe hyperphosphatemia, especially in the tumor lysis syndrome and particularly if symptomatic hypocalcemia cannot be adequately treated for fear of inducing widespread soft tissue calcification. Fasting or starvation does not lead directly to hypophosphatemia, apparently because phosphate is mobilized from catabolized bone and soft tissue in amounts sufficient to maintain serum phosphate, even during prolonged caloric deprivation. Therapy with the tyrosine kinase inhibitors imatinib and nilotinib appears to cause hypophosphatemia, at least in part, by inhibiting both osteoblast and osteoclast formation, lowering serum calcium and stimulating secondary hyperparathyroidism. The clinical picture is dominated by weakness, bone pain, and other features attributable to the associated rickets or osteomalacia (see Chapter 29). The pathogenesis of phosphate wasting that often follows partial hepatectomy or renal transplantation remains unclear, but humoral mechanisms seem to be involved. Hypophosphatemia in these situations is most pronounced when there is underlying phosphate depletion, as in hyperparathyroidism or vitamin D deficiency, or following prolonged malnutrition, alcoholism, or glycosuria. Accelerated uptake of phosphate into cells is particularly common in postsurgical, burn, or trauma patients, in whom it may be promoted by high levels of circulating catecholamines and exacerbated by concurrent respiratory alkalosis, fever, volume expansion, sepsis, and hypokalemia. Situations of greatly accelerated net bone formation, such as hungry bone syndrome occurring immediately following parathyroidectomy for primary or tertiary hyperparathyroidism, during initial treatment of severe vitamin D deficiency or Paget disease, or in occasional patients with extensive osteoblastic bone metastases, may manifest hypophosphatemia as well as hypocalcemia. Unfortunately, the status of the total-body phosphorus pool, and more particularly the critical intracellular pool, is reflected only indirectly by the concentration of phosphate in the extracellular fluid, which contains less than 0. Thus, although serum phosphate concentrations generally are used to characterize hypophosphatemia as severe (<11. Conversely, it may be low when intracellular phosphate is relatively normal, such as following a sudden movement of extracellular phosphate into cells. The prevalence of severe hypophosphatemia among hospitalized patients overall is less than 1%, whereas mild or moderate hypophosphatemia may be detected in 2% to 5%. Among the most common are various neuromuscular symptoms, ranging from progressive lethargy, muscle weakness, and paresthesias to paralysis, coma, and even death, depending on the severity of the phosphate depletion. Confusion, profound weakness, paralysis, seizures, and other major sequelae generally are limited to those with serum phosphate concentrations below 0.
Lamb Mint (Spearmint). Trileptal.
- Gas (flatulence), indigestion, nausea, sore throat, diarrhea, colds, headaches, toothaches, cramps, cancer, arthritis, muscle pain, and skin conditions.
- How does Spearmint work?
- What is Spearmint?
- Dosing considerations for Spearmint.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96820
In women who retain normal ovulatory cycles after having received cytotoxic chemotherapy and who spontaneously conceive no evidence of an increase in birth defects has been detected symptoms 2 days after ovulation 600 mg trileptal order. Recovery of ovarian function in amenorrheic women and the possibility of a premature menopause in women retaining a normal cycle are difficult to predict accurately following an insult to the gonads received during multimodality cancer therapy. Preservation of fertility in women who are to undergo intense treatment likely to result in infertility is a significant research growth area. Treatment of Hodgkin disease frequently includes local irradiation of involved lymph nodes, including those along the iliac vessels. The ovaries lie adjacent to the iliac vessels and will receive a dose of approximately 35 Gy, inevitably resulting in premature ovarian failure. Oophoropexy to remove the ovaries from the irradiation field, combined with shielding, can reduce the dose of irradiation received by the ovaries to less than 6 Gy, thereby reducing the incidence of amenorrhea by around 50%. Embryo storage requires the patient to be in a stable relationship and undergo controlled stimulation of the ovary for several weeks, along with regular ultrasonograph monitoring and aspiration of follicles. This technique is time-consuming when there is a pressing need to start treatment, is invasive, does not permit natural conception, and is not applicable to prepubertal girls. Oocyte cryopreservation is considered for patients without a partner; it requires stimulation of the ovaries and retrieval of the oocytes. Success rates have improved significantly in specialist reproductive centers, so this procedure should be considered where available. Interest has remained in cryopreservation of ovarian cortical strips rich in primordial follicles that can later be thawed and grafted back into the patient at the original site (orthotopic) or elsewhere (heterotopic). Several large centers are now storing ovarian strips, and to date over 20 live births following orthotopic regrafting in women surviving cancer have been reported. Only time will tell if this technique will further improve fertility prospects of women who undergo multimodality cancer therapy. In women under the age of 50 years who have developed gonadal failure the impact is twofold-fertility and sex steroid production. Sex steroid replacement is recommended to alleviate symptoms of hot flushes, mood changes, and vaginal dryness, as well as to prevent loss of bone mass. The recognition of the adverse effects of head and neck irradiation, particularly for secondary cancers, has led to the demise of radiation therapy for benign diseases, including acne vulgaris, goiter, tuberculous adenitis, thymic enlargement, and tonsillar hyperplasia. Use of low-dose (2-7 Gy) radiation therapy for benign disease was common in the United States from the 1930s through the 1950s. Following irradiation the prevalence of both thyroid dysfunction and formation of thyroid nodules increases significantly. In the first year after radioiodine therapy, several studies have reported increased rates of spontaneous and induced abortions. Doses of radioiodine used in treatment of thyrotoxicosis result in only minimal and transient changes in the germinal epithelium and Leydig cell function in men. In the majority of cases, patients presenting with subclinical hypothyroidism are likely to progress to overt hypothyroidism with time, and therefore, early intervention is warranted.
Specifications/Details
Cholesterol is necessary for the synthesis of estrogen medicine man dispensary 600 mg trileptal overnight delivery, progestins, androgens, aldosterone, vitamin D, glucocorticoids, and bile acids. Cholesterol deficiency is associated with severe developmental defects, as manifested in the rare SmithLemli-Optiz syndrome, which is likely caused by disruption of the Hedgehog signal transduction pathway. Fatty Acid Metabolism Fatty Acid Biosynthesis In humans eating a typical Western diet, the overall contribution of de novo lipogenesis to lipid metabolism is small because the ingestion of exogenous fat is sufficient to suppress the energy-requiring process of synthesizing fats from carbohydrates. However, high-carbohydrate diets, especially those containing fructose,6 substantially increase lipogenesis in liver and adipose tissue of humans. Most tissues carry out fatty acid biosynthesis to at least a small degree regardless of nutritional status. Malonyl CoA also serves as substrate for fatty acid synthase, which sequentially connects two carbon fragments to generate saturated fatty acids such as palmitate. Inhibition of fatty acid synthase in the hypothalamus suppresses appetite, inducing weight loss and improving insulin sensitivity. Here, -oxidation generates acetyl CoA, which can also be generated from glycolysis (bottom left). The acetyl CoA serves as a substrate for de novo synthesis of fatty acids, as depicted on the right side of the figure. Extreme production of ketones occurs in the setting of insulin deficiency and represents a threat to life. Defects in fatty acid oxidation are among the most common inborn errors of metabolism. Presentations include nonketotic hypoglycemia, liver dysfunction, and cardiomyopathy. Stored triglycerides are metabolized to yield the fatty acids that circulate in plasma through the action of three distinct lipases with separate substrate specificities. The monoglycerides, in turn, are acted on by monoglyceride lipase to yield glycerol. Fatty acids Triglyceride and Phospholipid Metabolism Dietary fat consists of triglycerides and phospholipids, which are digested in the stomach and proximal small intestine. Triglycerides are broken down into component fatty acids in part through the action of pancreatic lipase, which is activated by bile acids. Bile salts form micelles that acquire fatty acids and interact with the unstirred water layer of the intestine, where fatty acids are absorbed. Longchain fatty acids are taken up by enterocytes, re-esterified into triglycerides, and exported into the lymph as lipoproteins. Medium-chain (C10) fatty acids directly enter the portal vein to access the liver.
Syndromes
- Molasses
- Vomiting blood (occasionally)
- Colonoscopy every 10 years
- Those who have not received the HPV vaccine in the past should get a series of three shots.
- Blood tests to check for anemia, diabetes, inflammatory diseases, and possible infection
- Bruising around the eyes or widening of the distance between the eyes, which may mean injury to the bones between the eye sockets
Other incidental pancreatic islet macroadenomas should also be removed treatment non hodgkins lymphoma generic 300 mg trileptal free shipping, mainly because of the possibility that one might become malignant. These include infusion of calcium into selectively catheterized pancreatic arteries with measurement of insulin in right or left hepatic venous effluent. The glucagonoma syndrome consists of hyperglycemia, anorexia, glossitis, anemia, diarrhea, venous thrombosis, and a characteristic skin rash termed necrolytic migratory erythema (see Chapter 38). Palliation is often possible with surgery or another ablative procedure (see later). Some patients have responded partially to the somatostatin analogue octreotide, although an initial response has not predicted a long-term response. Of course, one oversecreting tumor is sufficient to dominate the clinical features. If a nonfunctioning tumor becomes malignant, its lack of symptomatic TumorsSecretingGlucagon,VasoactiveIntestinalPeptide, orOtherHormones rapid intraoperative insulin and glucose levels in serum91 or intraoperative insulin levels in fine-needle aspirates of a pancreatic tumor. Accurate localization of tumor and, in particular, identification of metastatic disease is critical for preoperative decision making. The multicentricity and variable size of these tumors stretch the limitations of radiologic techniques that have difficulty imaging tumors smaller than 1 cm in diameter. Endoscopic ultrasonography with or without needle aspiration of a pancreatic mass is useful for characterizing pancreaticoduodenal abnormalities but is a technically demanding and expensive option for the foreseeable future. With the exception of endoscopic ultrasonography, the current preoperative imaging methods are not able to image tumors confined to the pancreas and smaller than 1. This technique has become the primary approach for diagnosis of small insulinomas in most medical centers, although experience has been limited to sporadic tumors. This association has led some to recommend resection for all pancreaticoduodenal tumors larger than 2. Improvements in pancreatic surgical technique, however, have made it possible to excise smaller lesions surgically, although the benefit from doing this is less clear. Certainly there is no compelling evidence to suggest that surgical removal of small tumors, unless they produce a hormonal syndrome, improves overall outcome. Some urge removal of all detectable macroadenomas if removal would not be dangerous. Total pancreatectomy with a high rate of complications has been used for very large tumors. Pancreaticoduodenal neuroendocrine tumors are usually well differentiated and quite resistant to chemotherapy.
Related Products
Additional information:
Usage: q._h.
Tags: 150 mg trileptal buy with amex, generic trileptal 150 mg amex, buy generic trileptal 150 mg, trileptal 600 mg order
Customer Reviews
Rathgar, 64 years: Obstetric and neonatal outcome after oocyte donation in 106 women with Turner syndrome: a Nordic cohort study. Chelation of bile salts with cholestyramine, 4 g mixed with fluid three times a day, can relieve symptoms.
Abbas, 23 years: Stimulation of osteoprotegerin ligand and inhibition of osteoprotegerin production by glucocorticoids in human osteoblastic lineage cells: potential paracrine mechanisms of glucocorticoid-induced osteoporosis. Inhibin B is predominant in the follicular phase, as is inhibin A during the luteal phase.
Barrack, 35 years: The gene is expressed in the follicular cells, and the mutations that lead to haploinsufficiency are associated with an increased rate of follicular atresia. Low serum concentrations of 1,25-dihydroxyvitamin D in human magnesium deficiency.
Karrypto, 39 years: The Sertoli cells are the major cell type in the seminiferous cords in prepuberty and early puberty, but in the adult, germ cells predominate. As noted earlier, a number of stone disorders are inherited, making the family history an important component of the basic evaluation.
Moff, 60 years: DiGeorge syndrome may, in fact, be a neurocrestopathy, because ablation of the premigratory cephalic neural crest in chick embryos produces the same phenotype. Paresthesias or episodes of distorted sensation, such as pins and needles, tingling, coldness, numbness, or burning, often accompany the pain.
Topork, 58 years: The onset at puberty correlates better with bone age than with chronologic age, although bone age is not any better at estimating the onset of puberty in normal boys than is chronologic age and cannot be considered a highly accurate test. Update of guidelines for the use of growth hormone in children: the Lawson Wilkins Pediatric Endocrinology Society Drug and Therapeutics Committee.
Orknarok, 37 years: The efficacy and safety of duloxetine were evaluated in three controlled studies using doses of 60 and 120 mg/day over 12 weeks. All of these drugs require endogenous insulin secretion to lower plasma glucose concentrations, and insulin secretion declines appropriately as glucose levels fall into the normal range.