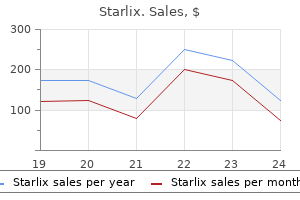
Only $1.09 per item
Starlix dosages: 120 mg
Starlix packs: 30 pills, 60 pills, 90 pills
In stock: 598
10 of 10
Votes: 109 votes
Total customer reviews: 109
Description
If the anteroposterior length of the skull is excessive acute primary hiv infection symptoms buy 120 mg starlix, some gentle compression can be applied by using absorbable plates and screws, but only if the width of the skull has been increased beforehand so that there is very little global pressure applied to the brain or the venous circulation. The bathyrocephalic skull will require removal and reshaping of the occiput, again using radial barrel stave osteotomies and flattening of the abnormal curvature with bone benders. A Lambdoid Synostosis Children with lambdoid synostosis typically have flattening of the parietal and occipital regions ipsilateral to the fused portion of the suture. If bilateral synostosis has occurred, symmetrical flattening of the occiput is seen. If the synostosis is severe, skull deformities in the frontal region, which may include elevation of the vertex of the skull, are evident. Mild to moderate forms with late closure of the suture rarely manifest obvious deformities from the frontal view and, as such, do not require surgical correction. OperativeTechnique Individualization of surgical technique is required; however, most deformities can be satisfactorily corrected with the patient in the prone position and surgical manipulations in the occipital bone. This discussion is restricted to patients having deformities in the parietal occiput. A biparietal occipital bone graft is elevated in patients with unilateral synostosis or bilateral lambdoid synostosis, with care taken to avoid injuring the transverse sinus. Barrel stave osteotomies are performed in both unilateral and bilateral synostosis; in bilateral lambdoid synostosis with bilateral posterior flattening, barrel stave osteotomies are performed to increase bilateral occipital projection. In patients with unilateral lambdoid synostosis, the occiput is fractured posteriorly, ipsilateral to the fused suture unilaterally, and inwardly on the contralateral bulging side. In unilateral synostosis, the convex side is made flatter, and the flatter side is made more convex with the use of greenstick fractures. In patients with bilateral lambdoid synostosis, a bilaterally convex occiput is achieved by similar means. The most serious problems associated with cranioplasty procedures are blood loss, air embolus, and infection. Prophylactic measures such as preoperative administration of erythropoietin or perioperative tranexamic acid, adequate blood and clotting factor replacement, and monitoring for blood loss are useful and necessary. Because of low circulating blood volumes in very young patients, it is imperative that attention is paid to achieving good hemostasis intraoperatively, and monitoring blood loss postoperatively. A, Posterior procedure, consisting of occipital craniotomy, parietal craniotomies, and removal of the lambdoid suture to allow forward movement of the occiput. Points "a" and "b" represent the two areas on the skull that come into contact once the intervening bone segment is removed when shortening the sagittal strut. A, Unilateral lambdoid fusion: unilateral fusion (1), occipital flattening (2), and anteriorly displaced ear ipsilateral to fusion (3). B and C, Bilateral lambdoid fusion with bilateral occipital flattening (4), prominence of frontal bone (5), and elevation of skull vertex (6). This possibility is anticipated by increasing the circulating volume at the outset of surgery; maintaining hypotension, but with a high circulating volume, during osteotomies of the cranial bones; and monitoring for air embolus with Doppler examination and carbon dioxide and nitrogen detection techniques. Early on, it was recognized that simple synostectomy was insufficient and that more extensive procedures produced better results.
Disodium Edetate (Edta). Starlix.
- Treating coronary heart disease (CHD) or peripheral arterial occlusive disease.
- Emergency treatment of life-threatening high calcium levels (hypercalcemia).Treating heart rhythm problems caused by drugs such as digoxin (Lanoxin).
- How does Edta work?
- Are there any interactions with medications?
- Dosing considerations for Edta.
- What is Edta?
- Treating corneal (eye) calcium deposits.
- Are there safety concerns?
- Treating lead poisoning.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96988
Variation in intracranial pressure monitoring and outcomes in pediatric traumatic brain injury what does hiv infection impairs generic 120mg starlix overnight delivery. Craniocervical arterial dissection in children: clinical and radiographic presentation and outcome. Pediatric neurocritical care: a neurology consultation model and implication for education and training. Emerging subspecialties in neurology: building a career and a field: pediatric neurocritical care. Length of stay and mortality in neurocritically ill patients: impact of a specialized neurocritical care team. Effect of implementation of a paediatric neurocritical care programme on outcomes after severe traumatic brain injury: a retrospective cohort study. Multimodal monitoring in traumatic brain injury: current status and future directions. Brain tissue oxygen monitoring after severe traumatic brain injury in children: relationship to outcome and association with other clinical parameters. Transcranial Doppler-based assessment of cerebral autoregulation in critically ill children during diabetic ketoacidosis treatment. Cerebral hyperemia measured with near infrared spectroscopy during treatment of diabetic ketoacidosis in children. The epidemiology of vasospasm in children with moderate-to-severe traumatic brain injury. Optic nerve sheath diameter as a marker for evaluation and prognostication of intracranial pressure in Indian patients: an observational study. Tissue oxygen index: thresholds for cerebral ischemia using near-infrared spectroscopy. Acute care clinical indicators associated with discharge outcomes in children with severe traumatic brain injury. Incidence of hypo- and hypercarbia in severe traumatic brain injury before and after 2003 pediatric guidelines. Cerebrovascular response in infants and young children following severe traumatic brain injury: a preliminary report. Part 1: relation to age, Glasgow coma score, outcome, intracranial pressure, and time after injury. Childhood arterial ischaemic stroke incidence, presenting features, and risk factors: a prospective population-based study. Intelligence after stroke in childhood: review of the literature and suggestions for future research. Neurologic outcome in survivors of childhood arterial ischemic stroke and sinovenous thrombosis. Report of the National Institute of Neurological Disorders and Stroke workshop on perinatal and childhood stroke.
Specifications/Details
The skull deformity in this type of synostosis has the most variability in the presentation and shape of the skull hiv infection by swallowing blood buy starlix 120 mg overnight delivery, depending on the exact location of the involvement along the sagittal suture and also on the timing of the sutural closure. An individually tailored surgical technique is necessary to address the most salient deformities. Usually, one of three varieties of sagittal synostosis predominates: anterior compensation, posterior compensation, and the "golf tee" or bathyrocephalic deformity. Milder cases can be successfully treated with removal of the fused sagittal suture and application of distraction devices, such as the spring cranioplasty, to gradually widen the skull. The neurological implications of the less comprehensive procedures are still concerning yet may have a role in specific cases, but the grading for what is a "mild" case still has not been defined. The sutures act as points of attachment to the underlying dura and, if not removed, will prevent the overlying bony skull from sliding over the dura during the reshaping process and will result in relapse of the original deformity. Release of the sagittal suture in particular often results in immediate and spontaneous widening of the entire calvarium as the restraining force of the fused suture is removed. The frontal bone is removed, especially when significant bossing is encountered, and then radial barrel stave osteotomies are performed and the bone is flattened with a bone bender to remove 3 1 4 OperativeTechnique As in children with bilateral coronal synostosis, patients with complete sagittal synostosis frequently have simultaneous evidence of deformity in the anterior and posterior skull. The anterior type is often accompanied by bilateral frontal bossing and is often the most noticeable or visible deformity. In the past, this was most commonly treated by a procedure or some modification thereof. A, Fusion of anterior portion of sagittal suture with compensatory frontal bossing. B, Fusion of posterior sagittal suture with compensatory occipital bossing and bathrocephaly. C, Golf tee deformity: narrowing of posterior occiput with posterior sagittal fusion, resulting in frontal bulge compensation, as viewed from above. An early unilateral coronal synostosis may not (but usually does) need a contralateral frontal correction to achieve an ideal result, but a bilateral coronal synostosis has a brachycephalic deformity that, in our experience, cannot be corrected without simultaneous extensive cranial remodeling, especially in the occiput, and distraction osteogenesis is particularly desirable in syndromic and redo surgical cases. The surgical techniques discussed in this chapter are not meant to be rigidly adhered to , but they should serve as a framework for the treatment of individual patients. Experimental alteration of cranial suture growth: effects on the neurocranium, basicranium and midface. Age as a critical factor in the success of surgical correction of craniosynostosis. Metopic and sagittal synostosis: intracranial volume measurements prior to and after cranio-orbital reshaping in childhood.
Syndromes
- Kidneys -- an infection of one or both kidneys is called pyelonephritis or a kidney infection.
- Hantavirus pulmonary syndrome
- Weakness
- Chromosome testing (may detect a chromosomal problem)
- One brand of vaccine can be substituted for another in the 3-dose series. The HPV vaccine can be given at the same time as other vaccines.
- Less pain.
- Chest discomfort or pain
- Foods from this group are excellent sources of B vitamins, protein, iron, and zinc.
- Minor scratches
- Eating something you are allergic to can cause nausea, vomiting, abdominal pain, cramping, diarrhea, or a severe, life-threatening reaction.
This increased incidence may account for unexplained hearing loss hiv infection europe starlix 120mg buy on line, tinnitus, and self-audible bruits in these children and poses a risk for difficultto-control bleeding at myringotomy. A retrospective study revealed increased mortality (in comparison to population standards) among achondroplastic children younger than 4 years; sudden death from brainstem compression was identified as the cause of half the deaths. Microcystic histopathologic changes, cervical syringomyelia, necrosis, and gliosis have been reported in autopsies of achondroplastic children who died unexpectedly; these findings may have been related to indolent, chronic compression and damage. White matter injury and secondary encephalomalacic degeneration within the brainstem may also be detected through the use of diffusion tensor imaging. We therefore consider infants with a history of sleep apnea or other severe respiratory or neurological abnormalities to be at increased risk for respiratory complications resulting from occult cervicomedullary compression. Some authors have recommended performing sleep and intracranial imaging studies on all children with achondroplasia. Hypotonia can appear as a symptom of cervicomedullary compression, and a delay in gross motor development and generalized hypotonia are common in achondroplastic children. Affected patients can present a striking contrast to the usual floppy, hypotonic achondroplastic infant. We use these studies to identify patients who are at risk for neurological damage or sudden death and then recommend treatment before abrupt and irreversible changes occur. For the purpose of diagnosis, clinically significant cervicomedullary compression warrants intervention when patients demonstrate (1) neurological evidence of upper cervical myelopathy (asymmetrical limb movements and reflexes, spontaneous or sustained clonus, failure to develop head/neck control with trunk and limb hypotonia) or of chronic brainstem compression (apnea, lower cranial nerve dysfunction, swallowing difficulties); (2) evidence of stenosis on imaging studies, including the absence of flow above and below the foramen magnum; and (3) an otherwise unexplained respiratory or developmental abnormality. They reported data on rates of medical complications at specific age intervals (see Table 2341). Hunter and coworkers emphasized the important role of surgery, primarily because progressive neurological symptoms continue into adulthood. Evaluation Once a patient at high risk with respiratory or neurological symptoms or signs has been identified, we advise comprehensive testing. Parents should be carefully interviewed about the health and medical history of their child, with an emphasis on respiratory symptoms. Respiratory evaluation should include evaluation of blood pH, a chest radiograph, and overnight polysomnography. Electrocardiography and echocardiography should be performed to search for cardiac evidence of chronic oxygen deprivation during sleep. A neurological examination for signs of brainstem compression, such as hyperreflexia, hypertonia, paresis, asymmetry of movement or strength, or abnormal plantar responses, is essential. Brainstem auditory evoked potential and upper extremity somatosensory evoked potential evaluation should be considered as an adjunct, especially in patients with normal results on neurological examination. We also strongly recommend Hydrocephalus ClinicalFindingsandPathology Hydrocephalus in an achondroplastic patient is probably secondary to deformation of the cranial base. Constriction of the basal foramina, particularly the jugular foramina, is thought to reduce venous drainage and potentially raise intracranial venous pressure. Investigators have demonstrated a correlation between the degree of venous narrowing at the jugular foramina and the degree of hydrocephalus in achondroplaasia. Hydrocephalus may resolve in some patients with continued growth of the skull base during puberty.
Related Products
Additional information:
Usage: p.r.n.
Tags: discount starlix 120mg online, 120 mg starlix purchase free shipping, buy starlix 120mg cheap, buy starlix 120mg visa
Customer Reviews
Real Experiences: Customer Reviews on Starlix
Eusebio, 32 years: Cerebral revascularization using omental transplantation for childhood moyamoya disease. Plastic surgery techniques can then be used at the time of the initial operation, to provide the most reliable repair and avoid future complications. In a review of a number of large series published before 2011 that described children with tumors of the spinal column, Wetjen and Raffel6 found that 53 of 156 tumors in the intradural extramedullary space were epidermoids or dermoids, 48 were nerve sheath tumors, and 17 were meningiomas.
Flint, 42 years: Devoid of recurrent single nucleotide variations, these tumors seem to display a CpG island methylator phenotype, whereby transcription silencing converges on targets of the polycomb repressive complex 2. Monopolar electrocautery is used to dissect and clear muscle and soft tissue until the bone of the mastoid eminence and digastric groove is seen. Accumulating evidence suggests that these aneurysms have aggressive natural histories, requiring their immediate and aggressive treatment.
Angar, 56 years: These decisions affect the patient, siblings, parents, and caretakers in profound ways, and a responsible neurosurgeon must be careful to differentiate what is known and understood from what is conjecture. Superselective catheterization and angiogram of the anterior cerebral artery (C and D) and the N-butyl cyanoacrylate embolization cast (A and B). Therefore, the clinician should perform the necessary study to make the diagnosis.
Marik, 52 years: All of these procedures are traditionally performed in a conscious patient, with use of local anesthetics and mild sedation to allow the patient to assist in optimal placement of the stimulating electrode. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Shunt infections may occur within the ventricle and shunt tubing, within the peritoneal cavity, or within the subcutaneous tissue of the wound surrounding the shunt hardware.
Bogir, 22 years: Her painful area was marked (hatched area) using a conscious pain-mapping procedure intraoperatively. In efforts to estimate the increased risk of developing malignancy as a result of neuroangiographic procedures, researchers rely on comparisons with larger databases of radiation exposure by assuming a linear, no-threshold relationship between dose and cumulative risk. The second cervical nerve exits from the cervical canal immediately adjacent and dorsal to the joint capsules.