Only $1.91 per item
Kamagra Gold dosages: 100 mg
Kamagra Gold packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills
In stock: 708
10 of 10
Votes: 293 votes
Total customer reviews: 293
Description
The terminology and criteria for diagnosis are the same as those applied in the lung erectile dysfunction symptoms age kamagra gold 100 mg buy line. The prognosis is generally poor, probably because of late detection of the tumor and lack of effective treatment. Microscopic Appearances Carcinoids are characterized by organoid clusters, sheets, and ribbons of polygonal cells separated by delicate fibrovascular stroma. True rosettes, pseudorosettes, perivascular rosettes, and spherical masses (often with comedo necrosis) can be present. The tumor cells possess round or oval nuclei with finely dispersed chromatin and inconspicuous nucleoli. Typical carcinoid is defined by a mitotic count of less than 2/10 hpf (2 mm2) and lack of necrosis. Atypical carcinoid is defined by (1) a mitotic count of 2 to 10/10 hpf (2 mm2) or (2) presence ## Carcinoid Tumor (Typical and Atypical) Clinical Features Carcinoid tumors of the thymus are uncommon. The patients have no symptoms, are initially seen with symptoms referable to the mediastinal mass, or have endocrine symptoms. A, Sheets of polygonal cells are traversed by delicate fibrovascular septa, characteristic of endocrine neoplasm. Pigmented variant, with ceroid pigment or melanin pigment being present in some tumor cells. This may mimic spindle cell thymoma, but the neuroendocrine nature of the tumor is suggested by the granular chromatin, granular cytoplasm, and delicate fibrovascular septa. The right field shows the component of atypical carcinoid, with eosinophilic granular cytoplasm. Thymic carcinoid with divergent sarcomatoid differentiation, with intermingling of the carcinoid with a sarcomatous component, which may even exhibit osseous or cartilaginous differentiation. Most tumor cells are positive for panneuroendocrine markers such as chromogranin and synaptophysin, in contrast to the patchy staining commonly observed in thymic carcinoma. The cytoplasm contains mitochondria, welldeveloped rough endoplasmic reticulum, and dense-core neurosecretory granules. Large cell lymphoma may simulate carcinoid tumor because of compartmentalization by a sclerotic stroma. In general, the tumor cells are more dispersed in at least some areas, and they commonly exhibit irregular nuclear folding. The diffuse subtype of carcinoid may simulate seminoma, but the latter often features prominent nucleoli, a sprinkling of lymphocytes, and lack of, or only focal dot-like staining for, cytokeratin. Paraganglioma shows a characteristic Zellballen pattern without formation of trabeculae. Lack of staining for cytokeratin and presence of S100-positive sustentacular cells around the tumor packets help to distinguish this tumor from carcinoid. Rare examples show focal squamous differentiation or adenosquamous differentiation. Teratomas are the most common, accounting for 44% of all cases and an even higher percentage in children (70%).
Side-Saddle Plant (Pitcher Plant). Kamagra Gold.
- How does Pitcher Plant work?
- What is Pitcher Plant?
- Dosing considerations for Pitcher Plant.
- Are there safety concerns?
- Digestive disorders, constipation, urinary tract diseases, fluid retention, preventing scar formation, pain, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96145
Tumors consisting entirely of signet ring cells have a worse prognosis than those admixed with another component erectile dysfunction causes cheap kamagra gold 100 mg fast delivery. Although cells with abundant clear glycogen-rich cytoplasm are common, they are not essential to the diagnosis, and some lesions have mainly, or entirely, flattened or hobnail cells. As referred to earlier, some urothelial carcinomas have prominent areas of glandular differentiation, and this is a much greater problem that is hugely dependent on sampling. In samples showing only adenocarcinoma, the possibility of urothelial carcinoma with glandular differentiation cannot be excluded without examination of the entire lesion. Immunohistochemistry may be of assistance, in that areas of glandular differentiation may retain expression of markers associated with urothelial carcinoma such as high molecular weight cytokeratin and p63. Some adenocarcinomas are very well differentiated, and architectural features may be more helpful than cytologic ones in establishing the diagnosis of carcinoma in these cases. The distinction may be especially difficult in cases of intestinal-type cystitis glandularis1; lack of cytologic atypia or muscle invasion is key in this regard. Adenocarcinoma should also be distinguished from the rare villous adenoma of the bladder. These lesions lack invasion, in contrast to adenocarcinoma, but this feature may not be evident in a limited biopsy specimen. It is advisable to have a lesion with that differential completely excised so that its invasive properties, or lack of them, can be discerned. Adenocarcinoma must also be distinguished from three other nonneoplastic lesions, endometriosis, endocervicosis, and endosalpingiosis. It should be noted, however, that in postmenopausal patients or patients who are being given treatment with hormones, the stroma may be atrophic and not discernible around every gland. The benign features of the epithelium in endometriosis and endocervicosis are also helpful in the distinction from adenocarcinoma. Endocervicosis may cause particular difficulty because it often forms a mass and lacks endometrial stroma and the epithelium is mucinous. As the glands of endocervicosis often are distributed haphazardly in the muscularis propria of the bladder, lack of familiarity with this entity may suggest the possibility of a deeply invasive, well-differentiated mucinous adenocarcinoma. Primary adenocarcinoma must be distinguished from spread of another adenocarcinoma to the bladder. The most common problem of this type is posed by invasion of the bladder by prostatic adenocarcinoma. In most cases, examination of routinely stained sections shows the characteristic small acinar or cribriform appearance of prostatic adenocarcinoma, which differs from that of most adenocarcinomas of the bladder. Even when a prostatic carcinoma has unusual histologic features, it typically stains positively for at least one of these antigens.
Specifications/Details
The number of cell layers is usually fewer than seven erectile dysfunction protocol free safe 100 mg kamagra gold, cytologic atypia is absent or minimal, and mitotic figures are absent or very rare and confined to the basal layer. The epithelial cells may show a variety of changes such as vacuolation, degenerative atypia, and an apocrinelike appearance of the cytoplasm Differential Diagnosis the papillae in typical papillomas may branch, but the particularly complex branching of many papillary carcinomas usually is not seen. Additionally, the papillae are usually covered by fewer than seven layers of urothelial cells, which is less than the urothelium covering the papillae in most papillary carcinomas. Finally, although a rare mitotic figure does not necessarily exclude the diagnosis of papilloma, significant mitotic activity strongly favors carcinoma. If the papillae are short and broader without a well-defined fibrovascular core, papillary hyperplasia should be considered. The average age of the patients, who typically have obstructive symptoms or hematuria, is about 57 years. No appreciable urothelial thickening is seen, and many umbrella cells are present. A polypoid nodule is covered by normal urothelium, underneath which are anastomosing trabeculae of basaloid-appearing cells. On gross examination they are typically solitary, polypoid, and variably smooth or lobulated. On the basis of their microscopic features, inverted papillomas have been divided into trabecular and glandular types. These are cellular tumors composed of anastomosing trabeculae and nests of urothelial cells, characteristically covered by normal urothelium. Peripheral palisading often imparts a resemblance to cutaneous basal cell carcinoma. Whorls suggestive of abortive squamous change may be seen, but frank squamous change with keratinization is uncommon. In contrast, the glandular type is characterized by nests containing spaces lined by mucinous epithelium. Inverted papilloma usually exhibits minimal cytologic atypia and mitotic activity but, in one report, 15% had "varying degrees of nuclear abnormalities and increased mitotic activity. Distinction between polypoid cystitis glandularis and the glandular variant of inverted papilloma is often arbitrary and of no clinical consequence. Differential Diagnosis Inverted papillomas must be distinguished from urothelial carcinoma that has an inverted pattern. Carcinomas that mimic inverted papillomas show a degree of cytologic atypia and mitotic activity incompatible with inverted papilloma and often have areas of more typical invasive carcinoma. Carcinoma with inverted architecture lacks the prominent peripheral palisading, maturation to the surface, and spindling of the cells of inverted papilloma. The presence of even a minor exophytic papillary architecture in a tumor with an inverting pattern suggests carcinoma.
Syndromes
- You have any new or unusual sores or spots on your skin
- Shaking or quivering sound to the voice if the tremor affects the voice box
- Neuroblastoma
- Hansen disease (leprosy)
- Medicines to treat symptoms
- Cerebral palsy
- Heart attack or stroke during surgery
- Gentamicin: 5 to 10 mcg/mL
- The person have trouble concentrating and may be unable to remember things. The person may be irritable, have headaches, dizziness, blurry vision, and nausea that comes and goes.
Globular inclusions (Russell bodies) or crystalline inclusions of Ig are not uncommonly seen in the cytoplasm of the lymphoplasmacytoid cells and plasma cells doctor's advice on erectile dysfunction discount 100 mg kamagra gold with amex. Rare cases are associated with numerous crystal-storing histiocytes, mimicking adult rhabdomyoma. Plasma cells are intermingled with small lymphocytes and lymphoplasmacytoid cells. An appreciable number of activated large cells are admixed with the lymphoplasmacytoid cells and plasma cells. Surface Ig can often be demonstrated as well, usually IgM+, IgD-, but sometimes IgM+ IgD+. The plasma cells in this example contain abundant crystalline immunoglobulin inclusions. Abundance of crystalline inclusions with identical appearance in a lymphoplasmacytic infiltrate strongly suggests a diagnosis of lymphoma over a reactive process. In general, a diagnosis of lymphoplasmacytic lymphoma should rarely be made in a mucosal site (for which a diagnosis of extranodal marginal zone lymphoma is more likely). Lymphoplasmacytic lymphoma can be recognized by the presence of many plasma cells and plasmacytoid cells. Plasmacytoma is composed of a monomorphous population of plasma cells instead of a mixed population of lymphocytes, plasma cells, and lymphoplasmacytoid cells. A small subset of patients with mantle cell lymphoma have no symptoms and have indolent disease. Sometimes, the neoplastic cells proliferate as broad mantles around residual reactive germinal centers, with coalescence and extension into the interfollicular regions. Scattered solitary epithelioid histiocytes are commonly present and constitute a helpful diagnostic clue. The blood vessels often show hyalinization, and thick reticulin fibers are commonly present. Their nuclei show variable degrees of indentation and angulation while usually maintaining an overall spherical configuration. In some cases, some tumor cells may have an appreciable amount of pale cytoplasm, mimicking monocytoid B cells. A single biopsy may shows areas with typical morphology and areas with blastoid appearance. Blastoid features may also appear in a subsequent biopsy of a patient with classic mantle cell lymphoma, and vice versa.
Related Products
Additional information:
Usage: q._h.
Tags: discount 100 mg kamagra gold otc, generic kamagra gold 100 mg buy online, discount kamagra gold 100 mg otc, 100 mg kamagra gold purchase with visa
Customer Reviews
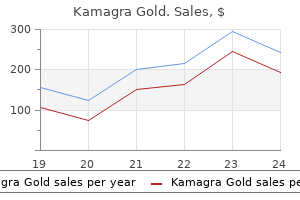
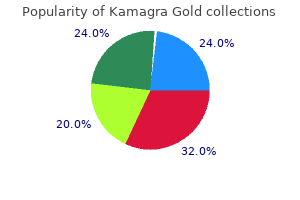
Real Experiences: Customer Reviews on Kamagra Gold
Chenor, 57 years: Bain G O, Danyluk J M, Shnitka T K 1985 Malignant fibrous histiocytoma of prostate gland. However, distinction from reactive lymphoid hyperplasia can be extremely difficult for cases predominated by small cells or showing a mixture of cells, especially when many admixed inflammatory cells are present. Hagood P G, Johnson F E, Bedrossian C W 1991 Small cell carcinoma of the prostate. In this illustration some glands have open lumina, but others are forming cords, seemingly with collapsed lumina.
Khabir, 38 years: A micropapillary pattern in which long, thin tufts of tumor cells grow into cystic spaces is also common. In most cases, undifferentiated carcinoma has spread beyond the ovary by the time of diagnosis and most patients cannot be debulked optimally. In many cases, prominence of collagenous stroma is seen, obscuring malignant glands. Young R H, Gilks C B, Scully R E 1991 Mucinous tumors of the appendix associated with mucinous tumors of the ovary and pseudomyxoma peritonei: a clinicopathological analysis of 22 cases supporting an origin in the appendix.
Torn, 62 years: Distinction between a signet ring cell carcinoma and a benign process is usually not difficult, although occasional nephrogenic adenomas have tiny tubules that simulate signet ring cells, rarely leading to confusion with signet ring cell carcinoma. Pathologic Features Stromal nodule is a well-circumscribed neoplasm that on initial inspection may be mistaken for a smooth muscle tumor; however, stromal nodules typically are softer and are yellow. It occurs mostly in adults in the sixth to eighth decades and predominantly in men, although rare cases have been described in children and adolescents. The latter cells have triangular-shaped or elongated nuclei and barely visible cytoplasm.
Harek, 30 years: Hum Pathol 16: 961-964 Southgate J, Slade P R 1982 Teratodermoid cyst of the mediastinum with pancreatic enzyme secretion. Bartholin Gland Adenoma (Adenomyoma) Bartholin gland adenoma36 is an extremely rare neoplasm that averages 2 to 3 cm in diameter, is solid, and often is 856 Vulva believed to be a cyst on clinical examination. It is important to differentiate primary tumors of the tube from secondary involvement by carcinomas arising elsewhere in the female genital tract or from an extragenital site. The neoplastic cells also tend to aggregate around residual lymphoid follicles and high endothelial venules.
Ortega, 32 years: Targeted Genetic and Whole Genome Sequencing High throughput nucleic acid sequencing technologies have allowed for the efficient survey of large numbers of genetic alterations in a single analysis. Other Benign Lesions Adenomyoma Although considered here as a variant of leiomyoma, whether adenomyomas53 represent a tumorous mass as opposed to a circumscribed variant of adenomyosis is not clear and this has not been studied pathogenetically. Evidence of the effects of screening in recent prostate cancer incidence, mortality, and survival rates. MalignantMesenchymalTumors Primary sarcomas of the urinary bladder are also uncommon.
Leon, 24 years: Hobnail cells are columnar and have either granular eosinophilic or clear cytoplasm. Exophytic papillae lined by neoplastic cells that have a combination of squamous and transitional features. Neoplastic rests are divided into adenomatous and nephroblastomatous types, based on cellular crowding and the prevalence of mitotic figures. Struma ovarii is composed of follicles filled with eosinophilic colloid and lined by cuboidal or columnar cells with uniform round nuclei.