Only $1.13 per item
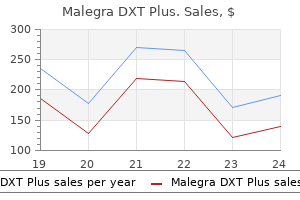
Malegra DXT Plus dosages: 160 mg
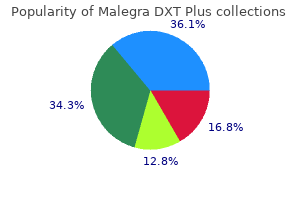
Malegra DXT Plus packs: 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills
In stock: 699
9 of 10
Votes: 156 votes
Total customer reviews: 156
Description
Neither an S3 nor an S4 gallop are likely given impaired inflow into the ventricular chambers erectile dysfunction treatment auckland discount 160 mg malegra dxt plus with amex. A square root sign is associated with constriction, although even in the setting of constriction plus tamponade this sign is absent while there is substantial fluid in the pericardial space because it depends on rapid inflow during early diastole. Lack of respiratory variation in Doppler inflow velocities across the tricuspid and mitral valves Answer: c. Chamber collapse in tamponade is caused by diminished transmural pressure, caused by rising intrapericardial pressure. Because pressures in the right-sided chambers are typically much lower than on the left, chamber collapse occurs much earlier on the right side, and may be caused by a variety of other factors as discussed in the text. Left atrial collapse after coronary artery bypass grafting is not uncommon and is associated with fluid surrounding the left atrium after open heart surgery. Left ventricular collapse is uncommon, even in tamponade, and when it does occur, it suggests very high intrapericardial pressure; it is highly specific. An electrocardiogram finding associated with tamponade and rarely seen with other conditions is: a. Low voltage is a very common finding, but it is seen in a wide variety of clinical settings, including pulmonary disease, infiltrative myocardial disorders, muscle loss from prior infarction, hypothyroidism, and others. Electrical alternans, on the other hand, is typically seen when the heart swings back and forth in a large pericardial effusion and is a relatively specific, although not sensitive, finding for tamponade. Pericardiocentesis can result in worsening hemodynamic status in patients with tamponade and: a. The presence of an intact pericardium may prevent exsanguination in all of these clinical settings. In respiratory decompensation with tamponade, intubation should be avoided if possible. Chest compression is usually ineffective because it does not significantly address the underlying pathology and is unlikely to allow a higher stroke volume to be ejected. Anxiety and tachypnea are a common occurrence with tamponade related to catecholamine release and low cardiac output; sedation may undermine one of the last remaining protective mechanisms for maintaining cardiac output and aeration. Patients need to maintain intracardiac chamber pressure; diuresis in acute tamponade is counterproductive in many cases because venous return is decreased. Intubation increases thoracic pressure, also decreasing venous return in the setting of tamponade intubation may cause sudden hemodynamic collapse. Volume loss may be loss of whole blood, plasma, or extracellular fluid or a combination of all three.
Creosote Bush (Chaparral). Malegra DXT Plus.
- Dosing considerations for Chaparral.
- Are there safety concerns?
- How does Chaparral work?
- Are there any interactions with medications?
- Arthritis, cancer, sexually transmitted diseases, tuberculosis, colds, skin conditions, stomach ailments (cramps, gas), weight loss, urinary and respiratory infections, and chicken pox.
- What is Chaparral?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96770
The effects of ventilatory pattern on hyperinflation impotence grounds for divorce states cheap malegra dxt plus 160 mg mastercard, airway pressures, and circulation in mechanical ventilation of patients with severe air-flow obstruction. Physiologic effects of positive end-expiratory pressure in patients with chronic obstructive pulmonary disease during acute ventilatory failure and controlled mechanical ventilation. Response of ventilatordependent patients to different levels of pressure support and proportional assist. Proportional assist ventilation, in acute respiratory failure: effects on breathing pattern and inspiratory effort. Adaptive support ventilation versus conventional ventilation for total ventilatory support in acute respiratory failure. Reduced breathing variability as a predictor of unsuccessful patient separation from mechanical ventilation. Following protocol: weaning difficult-to-wean patients with chronic obstructive pulmonary disease. Pharmacological and nonpharmacological management of delirium in critically ill patients. Sedation and weaning from mechanical ventilation: linking spontaneous awakening trials and spontaneous 54. Noninvasive positivepressure ventilation for respiratory failure after extubation. Many patients with airflow obstruction experience low levels of dyspnea until the tidal volume approaches the inspiratory capacity. Breaths taken from high chest volumes require more work to perform and inspiratory muscles are mechanically disadvantaged. Dynamic hyperinflation reduces the reserve between end-expiration and total lung capacity. Further increases of lung volume cannot be accomplished without encroaching on total lung capacity. Although secretion load, elevated airway resistance, and high tidal driving pressures all increase the breathing workload, dyspnea depends most directly on the workload-to-work capacity ratio. For hospitalized patients with massive obesity which one of the following is most correct Patients with massive obesity tend to collapse airways and gas trap upon assuming the horizontal position. The upward thrust of the abdominal pressure is reduced by assuming an upright posture, relieving the tendency for expiratory collapse. In patients who are passively inflated by volume-controlled mechanical ventilation, changes in gas trapping are best indexed by which one of the following
Specifications/Details
Comparison of morphine and methadone for prevention of postoperative pain in 3- to 7-year-old children erectile dysfunction treatment pdf malegra dxt plus 160 mg order otc. Patient-controlled analgesia in children and adolescents: A randomized, prospective comparison with intramuscular administration of morphine for postoperative analgesia. Comparison of patient-controlled analgesia with and without a background infusion after lower abdominal surgery in children. Patient-controlled analgesia with low dose background infusions after lower abdominal surgery in children. The safety and efficacy of parent-/nurse-controlled analgesia in patients less than six years of age. Subcutaneous cannulae for morphine boluses in children: Assessment of a technique. Recurrent hypoxemia in children is associated with increased analgesic sensitivity to opiates. Tolerance, withdrawal, and physical dependency after long-term sedation and analgesia of children in the pediatric intensive care unit. Continuous epidural bupivacaine-fentanyl infusions in children following ureteral reimplantation. Continuous epidural infusion of bupivacaine for postoperative pain relief in children. Lumbar and thoracic epidural anesthesia for urologic and upper abdominal surgery in infants and children. Postoperative dorsal epidural analgesia in the child with respiratory disabilities. Lower limb nerve blocks in children using unsheathed needles and a nerve stimulator. The influence of tape type and of skin preparation on the force required to dislodge angiocatheters. Infants tolerate spinal anesthesia with minimal overall autonomic changes: Analysis of heart rate variability in former premature infants undergoing hernia repair. Caudal morphine for postoperative analgesia in infants and children: A report of 138 cases. Spinal versus peripheral effects of adjunct clonidine: Comparison of the analgesic effect of a ropivacaine-clonidine mixture when administered as a caudal or ilioinguinal-iliohypogastric nerve blockade for inguinal surgery in children. The efficacy and safety of a clonidine/bupivacaine combination in caudal blockade for pediatric hernia repair. Comparison of a bupivacaine-clonidine mixture with plain bupivacaine for caudal analgesia in children. Caudal clonidine and bupivacaine for combined epidural and general anaesthesia in children.
Syndromes
- A stroke is an interruption in or blockage of the blood supply to any part of the brain. A stroke is sometimes called an infarct. Multi-infarct means that many areas in the brain have been injured due to a lack of blood.
- Your health care provider will tell you if you need to stop taking any medicines before you have this test.
- Phenobarbital: greater than 40 mcg/mL
- Difficulty breathing
- Irritation
- Electromyography
- Basophils
- Bleeding
- Sleep disorders
- Angiodysplasia of the GI tract
Some studies have found an increase in infection rates when ventriculostomies were left in place for longer than 5 days erectile dysfunction 23 malegra dxt plus 160 mg order amex,23,24,28 but more recent data reveal no significant reduction in infection rates when catheters were replaced before the fifth day. Hemorrhage at the time of placement occurs about 1% to 2% of the time and only rarely needs to be surgically evacuated. Another potential risk of ventricular catheter insertion is aneurysmal rebleeding40 after an 214 Pa rt 1 Critical Care Procedures, Monitoring, and Pharmacology acute subarachnoid hemorrhage. Likewise, the drain should be clamped and placed to monitor when changing position or during transport to avoid overdrainage, which may cause ventricular collapse and possibly subdural bleeding. The mechanism that does the actual pressure transduction is what is inserted into the patient; the system functions independent of head position and the monitor is zeroed once before it is placed. This feature also is a disadvantage because the transducer cannot be recalibrated to zero after insertion, although newer designs do not require zeroing. System accuracy compared with a ventriculostomy has been shown in the subdural space, brain parenchyma, and ventricles, although the parenchymal fiberoptic pressures may consistently exceed ventriculostomy pressures by nearly 10 mm Hg. Catheter Tip Strain Gauge the catheter tip strain gauge consists of a miniaturized solid-state pressure sensor mounted in a titanium case at the tip of a long, thin, flexible nylon tube. The transducer tip contains a silicon microchip with diffuse piezoresistive strain gauges that connect to tiny wires that travel the length of the tube. It can be incorporated into a ventricular catheter and used in any intracranial space. The sensor measures the volume or concentration of red blood cells and their velocity and generates a flow signal. Although laser Doppler flow does allow continuous measurements of perfusion, the sample volume is small (1 mm3) and only relative changes can be determined. These monitors can be placed at the bedside through a standard twist drill craniostomy or through a smaller opening made with a 2. The transducer is incorporated into the end of a tube and can be used alone or in combination with a ventriculostomy. Fiberoptic systems operate by projecting light through an optic fiber to a miniature, displaceable mirror in the catheter tip. The greatest advantage of fiberoptic catheters is that they do not require fluid coupling for pressure transduction, which avoids the problems of waveform dampening and artifacts from poor coupling. Because they do not require fluid coupling, there also is less opportunity for contamination. When hemoglobin is fully saturated with oxygen, arterial blood carries approximately 20 mL of oxygen per deciliter to the brain. The oxygen content of venous blood draining the brain varies and depends primarily on how much oxygen the brain extracts.
Related Products
Additional information:
Usage: q._h.
Tags: generic malegra dxt plus 160 mg buy on line, buy generic malegra dxt plus 160 mg on line, malegra dxt plus 160 mg online, 160 mg malegra dxt plus order
Customer Reviews
Real Experiences: Customer Reviews on Malegra DXT Plus
Sanuyem, 50 years: Although salicylate use in pediatrics has declined following recognition of its association with Reye syndrome, choline magnesium trisalicylate combines the analgesic properties of a salicylate with limited effects on platelet function, thereby allowing its use in patients with qualitative and quantitative platelet issues. In patients with significant lumbar pathology, the injectate will tend to follow the path of least resistance, often flowing toward the side opposite to the pathology (40).
Emet, 35 years: To prevent hemodynamic decompensation during decompression, intravascular volume should be restored, oxygen delivery should be normalized, and hypothermia and coagulation defects should be corrected. Memory, delusions, and the development of acute posttraumatic stress disorder-related symptoms after intensive care.
Ateras, 43 years: Because of many sensitive structures in the neck adjacent to the stellate ganglion, fluoroscopic imaging is recommended. If sensitivity is set too low, the ventilator will be triggered by any process that causes the airway pressure to drop below the set threshold.
Rathgar, 28 years: They contain an electrical heating coil that sits in the right atrium, which heats up the blood in a semirandom binary fashion. A 25-year-old man sustains a stab wound to the upper abdomen with omentum visible on examination.
Rune, 27 years: Use of anticoagulants or drugs affecting platelet adherence may increase the risk (see Chapter 12). Evaluation of safety and effectiveness of standardized antifactor Xa-based unfractionated heparin protocols in obese versus non-obese patients.
Marius, 44 years: B, Mechanical ventilators monitor all the ventilation parameters, allowing both closedloop control of the generated waveform and providing information to the clinicians. The most frequent cause of renal hypoperfusion is hemodynamic compromise from septic shock, hemorrhage, hypovolemia, trauma, and major operative procedures.