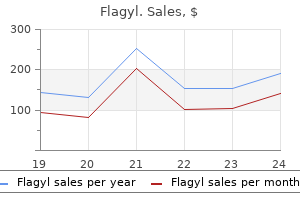
Only $0.22 per item
Flagyl dosages: 500 mg, 400 mg, 250 mg, 200 mg
Flagyl packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 739
9 of 10
Votes: 318 votes
Total customer reviews: 318
Description
Two studies have reported a polymorphism of the type 2 hypocretin receptor gene in association with cluster headache antibiotic chart 200 mg flagyl order with amex, although this was not replicated in a third multinational study. The use of the current term cluster headache is attributed to Encyclopedia of the Neurological Sciences, Volume 4 doi:10. However, a causative link to smoking has not been proven and seems unlikely, as smoking cessation does not seem to alter the clinical course of the disorder and cannot easily account for the disorder in children. The natural course of cluster headache can be difficult to predict, with some people showing a bidirectional transition between the episodic and chronic forms of the condition. Less frequent bouts of attacks and more prolonged, and sometimes permanent, periods of remission can occur with advancing age. The pain is typically focused in the distribution of the ophthalmic branch of the trigeminal nerve, behind the eye, over the temple or over the maxilla, although it may extend to other areas of the head and the neck. The vast majority of patients describe a sense of restlessness and agitation during an attack and will often pace, rock back and forth, and bang their heads. Photophobia may be reported, often limited to the same side as the pain, with fewer reporting an aversion to loud noise or strong smells during the attack. Aura phenomena, similar to those experienced during migraine, including visual phenomena and paresthesia, preceding the attacks by up to 60 min, have been described in a small minority of patients. Patients commonly have tenderness and cutaneous allodynia at and around the site of pain between attacks, including over the ipsilateral greater occipital nerve. Attack Duration and Frequency Attacks typically last between 15 and 180 min, although on rare occasions they can last longer. In a case series of British patients, a mean untreated minimum duration of 72 min and maximum duration of 159 min was reported. The onset of pain is rapid, and the sensation increases from serious discomfort to excruciating pain over the course of a few minutes. The pain usually stays at maximal intensity for the duration of the attack, although it may wax and wane slightly, or be punctuated by superintense stabs of pain. Cranial Autonomic Symptoms and Other Features Each attack is accompanied by one or more cranial autonomic symptoms or signs on the same side as the pain. Just over a third of patients report an often highly predictable time of onset during the day, with three quarters reporting attacks occurring at predictable times during the night, awakening them from sleep. However, patients may go for several years without a bout (up to 20 years in some cases), and others may have more frequent bouts each year. The onset of bouts can be very regular in some individuals, with spring and autumn months being particularly noted for bout onsets, which is potentially related to the changes in day length. Precipitants Small quantities of alcohol will precipitate an attack in the majority of sufferers, usually within an hour of ingestion. In three quarters of patients, attacks are related to nocturnal sleep, with daytime naps also being triggers in some.
Cineraria Maritima (Dusty Miller). Flagyl.
- Are there any interactions with medications?
- How does Dusty Miller work?
- Are there safety concerns?
- What is Dusty Miller?
- Dosing considerations for Dusty Miller.
- Migraine headache, vision problems, and improving menstrual flow.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96342
The profile of molecules that are overproduced in a given syndrome may be predicted from the level at which the enzymatic arrest occurs as flux through the pathway is stimulated by diminished negative feedback antibiotics for acne stopped working discount flagyl 200 mg amex. In those porphyrias where the principal site of production appears to be in the liver, including the acute porphyrias and porphyria cutanea tarda, fluctuations through the biosynthetic pathway as a result of regulatory effects from environmental or endogenous factors can occur very rapidly; indeed minute-to-minute oscillations in biosynthetic haem fluxes have been recorded in the liver. Thus, in starvation and on challenge with xenobiotic reagents (which place a demand for the production of haem to meet the needs for new cytochrome formation), as well as with endogenous hormonal changes, enhanced flux through the pathway leads to toxic overproduction of 5-aminolaevulinic acid. By the same token, rapid repression of the haem biosynthetic pathway in the liver can be induced by the administration of exogenous haem, a useful agent in the control of acute attacks and which rapidly corrects the disturbed metabolism (see next paragraph). Nonetheless, in patients with erythropoietic porphyrias such as congenital porphyria, enhanced rates of red cell destruction when hypersplenism supervenes or in response to light exposure greatly exacerbate the overproduction of porphyrin intermediates and aggravate photosensitivity due to increased porphyrin release. Short-term experiments indicate that exogenous haem may partially repress the endogenous haem biosynthetic pathway in erythroid tissue, but this has not proved to be useful for long-term relief in the erythropoietic porphyrias. Blood transfusion to suppress erythropoiesis or definitive replacement of bone marrow by transplantation has, however, proved to be successful in controlling the devastating manifestations of congenital erythropoietic porphyria. For clinical purposes, however, a useful operational definition of the porphyric syndromes distinguishes the acute from the nonacute porphyrias. The incidence of symptomatic acute intermittent porphyria was similar in all countries (0. Higher figures have been reported in other studies: one in Norway gave the prevalence of acute intermittent porphyria to be approximately 4 in100 000, with an overall annual incidence of 0. Acute variegate porphyria is most common in the Afrikaner population of South Africa: traced to a Dutch settler in the 17th century, it has a prevalence of about 3 in 1000 persons. There are isolated reports of high prevalence among the potters in the Bikaner district of Rajasthan, India. Nonacute porphyrias the most common condition in this category is porphyria cutanea tarda, with an estimated prevalence of approximately 1 in 10 000 in Norway. Protoporphyria, the second most frequent of the nonacute porphyrias, in which systemic features with cholestatic liver disease are rare (5%), is estimated to have a frequency of 1 in 75 000 to 1 in 200 000 births. Nonacute porphyrias are characterized by photosensitivity syndromes due to overproduction of macrocyclic porphyrins which cause light-induced skin injury. Several of the acute porphyrias may also cause overproduction of porphyrin intermediates that are either intrinsically fluorescent or readily oxidized to become fluorescent. These porphyrias may at times be accompanied by marked photosensitivity and blistering skin reactions, which are usually exacerbated during the acute attacks. Difficulties arise because there are many types of porphyria and, being rare, often episodic, and of low penetrance, they frequently escape formal diagnosis. It is also regrettable that biochemical complexity and scientific nomenclature intimidates many practitioners. These considerations also impede proper management, especially since costly technological sophistication and specialist referral is often needed for definitive diagnosis. Patients referred with skin manifestations to dermatologists are more readily identified, but the associated or subsequent neurovisceral manifestations in underlying porphyrias such as variegate or coproporphyria are not always recognized in the nonacute clinical context.
Specifications/Details
Patients with recurrences may be offered repeat Gamma Knife radiosurgery infection 400 mg flagyl purchase, microvascular decompression, or a percutaneous treatment option. Advantages of microvascular decompression include higher long-term success rates and significantly lower rates of facial dysesthesias. The trigeminal nerve is inspected for the evidence of compression and freed of arachnoid adhesions. Pieces of shredded Teflon are used to elevate compressive vascular structures away from the trigeminal nerve. The complications of microvascular decompression include cerebral or cerebellar infarction, hearing loss, facial paresis, facial dysesthesia, cerebrospinal fluid leakage, and pseudomeningocele formation. Introduction One of the most important developments in the field of neurology during the decade of the 1990s was the emergence of a novel type of genetic mutation as the cause of a large number of inherited neurodegenerative diseases. At first glance, this list may appear unwieldy or random, as a wide range of pathologies and 10 different nucleotide repeat sequences are represented. However, repeat disorders can be divided into four mechanistic categories, which reflect the sequence composition of the repeat and the location of the repeat within a gene. Gain-of-function due to production of a protein containing a polyglutamine tract expansion. Gain-of-function due to production of a protein containing a polyalanine tract expansion. Despite the fact that much progress has been made in understanding the pathogenic mechanisms underlying repeat expansion disorders, many questions remain to be answered before we know exactly how repeat expansion mutations cause inherited human diseases. Therefore, the proposed classification scheme is at risk of becoming outdated in future. Loss-of-Function of the Gene Containing the Repeat There are multiple repeat expansion disorders that result in a loss-of-function of the protein containing the repeat. Affected patients have a mild physical phenotype with macrocephaly, long face, and long ears. Three disorders caused by short polyalanine expansions (oculopharyngeal muscular dystrophy, cleidocranial dysplasia, and synpolydactyly) are not included in the trinucleotide repeat expansion disease category as the trinucleotide repeats responsible for these disorders are quite short and do not show the feature of genetic instability. In both cases, this hypermethylation silences the promoters, resulting in absent or decreased expression. Among Caucasian populations, it occurs at a frequency of 1 in 50 000, but is relatively uncommon in other racial groups. Patients typically show gait and limb ataxia, with limb weakness and depressed lower extremity tendon reflexes.
Syndromes
- Infection (a slight risk any time the skin is broken)
- Tube through the mouth into the stomach to wash out the stomach (gastric lavage)
- Discharge from the nose that has a bad smell, comes from only one side, or is a color other than white or yellow
- Low or unstable blood pressure
- Burns
- Excessive bleeding
- Constant discomfort
- Do you have any other symptoms?
- If you cannot find the object, grasp the lower eyelid and gently pull down on it to look under the lower eyelid. To look under the upper lid, you can place a clean cotton-tipped swab on the outside of the upper lid and gently flip the lid over the cotton swab.
Development of liver metastases is associated with subsequent death from tumour antibiotics for acne cons flagyl 400 mg order without a prescription, and surgical resection of the primary gastrinoma can reduce the incidence of liver metastases. Surgical intervention can also normalise gastrin levels and lessen the requirement for long-term medical therapy. Normalisation of gastrin levels may be an important additional benefit since long-term hypergastrinaemia had been associated with the development of gastric carcinoid tumours. These results lend further support to early surgical intervention in gastrinoma as well as aggressive surgical resection of limited hepatic metastases. Non-invasive tumour-localising studies Initial tumour localisation studies should be noninvasive and should adequately assess the liver for metastases. Extra-abdominal false-positive localisation studies were more common than intra-abdominal false-positive scans and were attributed to thyroid, breast or granulomatous lung disease. Invasive tumour-localising modalities Although non-invasive imaging studies are important to exclude unresectable metastatic disease, these studies may fail to image the primary gastrinoma. Invasive modalities may be useful to localise the primary tumour prior to surgery. This allowed identification of the arterial distribution containing the gastrinoma. Surgery for tumour eradication If preoperative imaging studies reveal no evidence of unresectable metastatic disease, then patients with sporadic gastrinoma and acceptable risk should undergo abdominal exploration for tumour resection and possible cure. Operative approach the surgeon should be prepared for hepatic resection if unsuspected liver metastases are identified intraoperatively. An upper abdominal incision that provides adequate exposure for exploration of the entire pancreas, regional lymph nodes and liver is necessary. The abdomen is initially inspected for metastases, with particular attention to possible ectopic sites of tumour such as the ovaries, jejunum and omentum. All suspicious hepatic lesions must be either excised or biopsied to exclude malignant gastrinoma. Similarly, hilar, coeliac and peripancreatic regional lymph nodes are carefully sampled for metastatic disease. Successful intraoperative localisation and resection of tumours may be extremely challenging because gastrinomas only 2 mm in diameter may reside in the wall of the duodenum. There is also a high rate of associated lymph node metastases and even the posibility of primary gastrinomas arising within lymph nodes. Successful intraoperative tumour identification requires knowledge of where primary gastrinomas arise. The head of the pancreas and duodenum are first exposed by mobilising the hepatic flexure of the colon out of the upper abdomen and dividing the gastrocolic ligament to open the lesser sac. A Kocher manoeuvre is performed to lift the head of the pancreas out of the retroperitoneum. The entire pancreatic surface is carefully examined visually and palpated between the thumb and forefinger.
Related Products
Additional information:
Usage: b.i.d.
Tags: buy generic flagyl 250 mg on-line, discount flagyl 500 mg overnight delivery, order flagyl 500 mg free shipping, cheap flagyl 400 mg fast delivery
Customer Reviews
Lisk, 25 years: The photosensitivity worsens under these circumstances and there is upper abdominal pain with splenic enlargement, jaundice, and extreme photosensitivity as concentrations of free protoporphyrin in the plasma rise. The myelin membranes originate from and are part of the oligodendroglial cell membrane. The oldest known patients are close to 40years of age, bedridden, and severely disabled. A visual field defect for red may betray the presence of a lesion when the fields for white stimuli are full.
Kalesch, 61 years: Long-term use of granulocyte colony-stimulating factor is associated with a number of complications and should be supervised by a haematologist. Transthoracic echocardiography can provide evidence of poor left ventricular function and, rarely, left ventricular thrombi. Affected infants may appear normal at birth, but by the first month of life fail to thrive; they develop steatorrhea, abdominal distention, and growth retardation due to fat and fat-soluble vitamin malabsorption. Muscle sympathetic activity reflects vasoconstrictor outflow and is strongly baroreflex dependent, whereas skin sympathetic activity includes vasomotor and sudomotor outflows and is affected by thermoregulatory and emotional influences.
Larson, 36 years: Endarterectomy and anatomical bypass are associated with far higher morbidity and mortality rates than other surgical and endovascular methods. May come to light at any age with postprandial abdominal pain and vomiting, symptomatic hypoglycaemia (which may induce seizures), hypophosphataemia, acidosis, and other metabolic disturbances after consumption of offending foods and drinks. It is composed of sensory fibers arising from the tibial nerve at the popliteal fossa, supplemented by fibers from the common peroneal nerve. Diagnosis is supported by suppression of aldosterone to undetectable levels during a low-dose dexamethasone suppression test (0.
Aila, 28 years: Status Epilepticus 299 seizure-stopping mechanisms, or the occurrence of a strong excitatory stimulus, may result in repeated or prolonged seizures. Perioperative steroids need to be given and the patient warned of the need for lifelong steroid replacement. Viral diseases have had a major effect on history, causing more deaths than all wars combined. Differential diagnosis and diagnostic assessment An abridged differential diagnosis is provided in Table 2.
Finley, 27 years: The release of adhesion at the trailing edge of the neuron involves regulation and internalization of cell adhesion molecule. They converge to a compact band called the internal capsule, which is flanked medially and laterally by nuclear masses, and they enter the crus cerebri (cerebral peduncle) in the upper brainstem, continue in the corticospinal tracts, and finally reach the pyramid in the lower brainstem. One of the virtues of proper handling of complaints is that they often show that although things did not turn out for the best, the problems that occurred were within the boundaries of those experienced in medical care and were not a sign of negligence. Every laboratory must have an established internal incident reporting system as part of Total Quality Management.
Esiel, 39 years: Prognosis the acute manifestations of galactosaemia and growth failure respond quickly to dietary therapy and cataract formation is prevented; in the early phases in the neonatal period, prompt intervention can lead to complete regression of cataracts. He investigated the toxicology of hemlock and other poisonous plants and minerals. Astrocytic tumors that are grades 1 and 2 are generally classified as astrocytomas, those that are grade 3 are classified as anaplastic astrocytomas, and those that are grade 4 are classified as glioblastomas. Blocking electrical activity can inhibit development of dendrites in the postsynaptic neuron, and this can lead to death of the postsynaptic neuron.