Only $0.52 per item
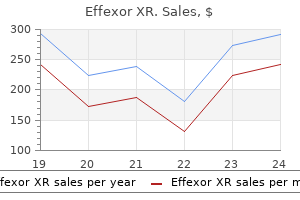
Effexor XR dosages: 150 mg, 75 mg, 37.5 mg
Effexor XR packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 733
10 of 10
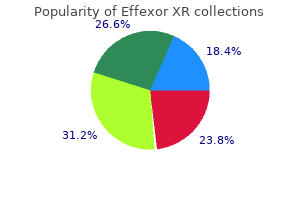
Votes: 160 votes
Total customer reviews: 160
Description
Myelinated fibres are distinguished further by their generally much larger calibre anxiety symptoms stomach 37.5 mg effexor xr buy free shipping, having diameters in the range 220 m in human peripheral nerves. Unmyelinated axons are always of small diameter and pass through the nerve trunk in groups of 815 within a common chain of Schwann cells. Nerve fibres have been classified according to their calibre into three groups: A, B and C (Table 24. Vasculature of Peripheral nerves Peripheral nerves are supplied by branches from their local regional blood vessels that ramify and branch within the epineurium. Pre-capillary vessels penetrate the perineurium at an oblique angle and are ensheathed for a short distance within the endoneurial compartment by internal prolongations of the innermost layers of the perineurial sheath. They then divide to supply the endoneurial plexus, which appears to consist nearly exclusively of capillaries. The plexus has a predominantly longitudinal orientation and drains directly to collecting blood vessels situated outside the perineurium, with few smooth muscle containing venules being found within the endoneurium. The contacts between the edges of adjacent capillary endothelial cells of the endoneurial circulation are completely sealed by tight junctions, and, in most species, this arrangement provides a second and effective barrier to the penetration of higher-molecular-weight materials into the endoneurial compartment. This bloodnerve barrier is, transmission of the nerve Impulse the most significant axonal function is its capacity to transmit signals over considerable distances in the form of propagated action potentials. The principal partitioned ion is sodium, and this is pumped outwards into the extracellular space. The advance of current through the axoplasm causes depolarization of adjacent segments of the axolemma, resulting in a continuously propagated wave of depolarization, which spreads along the axon. In unmyelinated fibres, the large capacitance of the axon membrane attenuates forward axial flow of current within the axoplasm and limits conduction to a speed of around 1 m/s. In myelinated fibres, on the other hand, electrical activity is restricted to the narrow spaces between the myelin segments, the nodes of Ranvier (The Internode and Node of Ranvier, see p. The principal functional implication of this saltatory activity is a considerable enhancement of conduction velocity in myelinated fibres over that achieved by nonmyelinated fibres, i. Loss of one or more myelin segments from a myelinated axon, as a consequence of either naturally occurring pathology or localized experimental injury, results acutely in conduction block, but the axon subsequently develops the capacity to sustain continuous conduction, in a manner comparable to that seen in normal unmyelinated fibres. Because of its great length (which may exceed 1 m in nerves to and from the human lower limb), when compared with the dimensions of the cell soma, the axonal cytoplasm, in most instances, contributes by far the largest component to the total mass of the neuron. Neurofilaments, microtubules, mitochondria and smooth endoplasmic reticulum are present, but there is no rough endoplasmic reticulum or Golgi apparatus. The smallest of the axoplasmic constituents that can be distinguished morphologically are microfilaments 57 nm in diameter, each of which is thought to be composed of paired helical chains of actin. They appear to be homologous with the thin filaments of muscle cells and contribute approximately 10 per cent to the total complement of 24. They are most conspicuous in the growth cones of actively elongating neurites and are less evident in unmyelinated axons and in the internodal portions of myelinated axons, where they appear to be confined to the cortical zone of axoplasm immediately subjacent to the axolemma. They may have contractile function and play a part in the mechanisms responsible for intra-axonal transport, growth cone motility and axon guidance. These are longitudinally oriented filaments of 811 nm in diameter, 1420 Chapter 24 Diseases of Peripheral Nerves linked by ill-defined lateral interconnections of a less dense axoplasmic component into an irregular polygonal lattice.
EPs 7630 (South African Geranium). Effexor XR.
- What is South African Geranium?
- Tonsillopharyngitis.
- Are there any interactions with medications?
- Are there safety concerns?
- Dosing considerations for South African Geranium.
- Bronchitis.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97079
Preferentially affects women in the fifth or sixth decade of life and children younger than the age of 10 years; gender ratio 5:1 femalemale anxiety and high blood pressure 75 mg effexor xr purchase free shipping. Antibodies to extracellular matrix protein-1 and T cells with receptor rearrangement point to an autoimmune pathogenesis. Anogenital manifestations cause severe discomfort (pruritus, dyspareunia, dysuria, and painful defecation) and present with polygonal papules and porcelain-white plaques, erosions, and various degrees of sclerosis. Vulvar lichen sclerosus is associated with an increased risk of squamous cell carcinoma; the role of human papillomavirus infection or prior radiotherapy remains to be elucidated. Potent topical corticosteroids and skin care are the most successful therapeutics; calcineurin antagonists have also recently demonstrated benefit. Evidence for the presumed infectious cause, such as acid-fast rods, spirochetes, or Borrelia, has not been found. There was no clinical and family history of autoimmune diseases or autoantibodies in the children studied. Of note, vulvar disease seems to have an increased risk of squamous cell carcinoma, but the role of additional cofactors. It preferentially affects women in the fifth or sixth decade of life and children younger than the age of 10 years. Early sclerosis and significant hemorrhage on the glans in early lichen sclerosus. Sclerosis of the frenulum and increased vulnerability with bleeding upon sexual intercourse. Significant sclerosis of the glans and conglutination with the preputium in advanced lichen sclerosus. In addition to the well-demarcated white vulvar plaque that is classic for lichen sclerosus, the waxy and crinkled texture, purpura (small arrows), and erosions (large arrow) are diagnostic. Sclerotic vulva with disappearance of the smaller labia and shrinkage of the introitus. Significant erythema and erosions are seen on the vulva and the anus in a figure-8 configuration. Blisters (occasionally hemorrhagic) may develop when the lichenoid infiltrate separates epidermis from the sclerotic dermis. Gradual obliteration or synechiae of the labia minora and clitoris, as well as stenosis of the introitus, may also result (see Chapter 78). Extragenital manifestations typically affect the thigh, the neck, trunk and lips; lesions are usually asymptomatic. A recent clinical histopathological study has revealed 27 adult cases with lip involvement. High-resolution ultrasound is occasionally used to document the depth of sclerosis. Collagen fibers are homogenized in the papillary dermis, and a lichenoid lymphocytic infiltrate is present. Morphea represents a circumscribed connective tissue disease with a number of different presentations.
Specifications/Details
However anxiety tremors order 75 mg effexor xr with amex, unless a general consensus concerning the implementation of molecular parameters into the routine classification of these neoplasms is achieved, classification should still primarily rely on histological features, bearing in mind that morphological criteria leave considerable space for subjectivity and interobserver variability. Thus, at present, the diagnosis of oligoastrocytoma remains controversial and more objective genetic or epigenetic parameters are needed to improve the classification of such neoplasms (Box 28. The role of quantitative assessments of each cytological component in oligoastrocytomas is disputed because precise percentages are difficult to determine given limited tumour sampling and the presence of tumour cells with ambiguous phenotypes. An older study reported that patient survival was similar irrespective of whether oligodendrocytes or astrocytes predominated or whether the proportion of these two cell types was approximately equal. One study reported that patients with histologically low-grade oligoastrocytoma but a Ki67 labelling index of 10 per cent showed a reduced time to progression that was similar to that of anaplastic oligoastrocytoma patients. Only tumours with an additional classic astroglial component should be diagnosed as oligoastrocytoma. Molecular analyses, in particular testing for 1p and 19q, is often performed to supplement the diagnostic and prognostic assessment of oligoastrocytomas or diffuse gliomas with ambiguous histology, and may indeed assist therapeutic decision making in progressive and anaplastic oligoastrocytomas concerning the best type of adjuvant treatment. Immunohistochemistry There is no immunohistochemical marker that can reliably distinguish the astrocytic and oligodendroglial components in oligoastrocytomas. Approximately one third of the oligoastrocytomas demonstrate strong nuclear Anaplastic Oligoastrocytoma 1687 histogenesis the histogenesis of human oligoastrocytomas is unclear. The observation of common genetic alterations in the different histological components of individual tumours are consistent with oligoastrocytomas arising from a glial precursor cell able to undergo bipotential differentiation. An oligodendrocyte/type 2 astrocyte (O2A) progenitorlike cell might be a good candidate for the cell of origin in both oligodendrogliomas and oligoastrocytomas, but this remains speculative. In addition, epigenetic events and regional changes in the tumour microenvironment. Several studies suggest that oligoastrocytoma follows a clinical course intermediate between that of oligodendroglioma or diffuse astrocytoma. Molecular genetics the molecular genetic changes observed in oligoastrocytomas either correspond to those commonly present in oligodendrogliomas, i. Molecular analyses of microdissected oligodendroglial and astrocytic regions revealed common genetic alterations in most instances, indicating a monoclonal origin of both components. Incidence, age and sex distribution Data on the incidence of anaplastic oligoastrocytomas are sparse and confounded by the variability in the histological classification of these tumours. In their series of 987 patients with oligodendroglial, mixed or astrocytic tumours, only 11 (1. Most anaplastic oligoastrocytomas are primary tumours that present with a short clinical history. However, tumours may also develop by progression from pre-existing low-grade tumours. Undefined margins and inhomogeneous T1/T2 signals were found more commonly in anaplastic than low-grade oligoastrocytomas. Microscopy shows a diffusely infiltrating oligoastrocytoma with focal or diffuse histologic signs of anaplasia.
Syndromes
- Lack of energy
- Epididymitis
- Use of certain medications such as phosphate-containing laxatives
- Metallic taste in mouth
- Blood chemistry tests
- Coma
- Tobacco smoking
- Respiratory infections
- Babbles
- Neck swelling
Muscle at birth contains a high proportion of satellite cells typically 30 per cent but this decreases to around 5 per cent in adult life anxiety wrap for dogs safe 75 mg effexor xr. Ultrastructurally, satellite cells have nuclei with dense peripheral heterochromatin and a small volume of cytoplasm that contains few organelles, free ribosomes, rough endoplasmic reticulum, glycogen, microtubules and intermediate filaments. Most muscles, with the exception of some craniofacial and oesophageal muscles, are derived from the somites. Genetargeting experiments in the mouse define a transcriptional hierarchy in which the paired-domain transcription factors 25 25. These myotubes have large central nuclei with a prominent nucleolus, and scattered myofibrils. Early primary myotubes are initially clustered within a common basal lamina, but as differentiation continues each becomes surrounded by its own basal lamina. Secondary myotubes arise from successive waves of fusion of post-mitotic myoblasts, along the surface of the primary myotubes. These initially form within the vicinity of innervation sites on the primary myotube, and early secondary myotubes are at first encased within the same basal lamina as the parent primary myotube. With increased maturation, these secondary myotubes separate and attain their own basal lamina. Fibre typing, particularly with antibodies to myosin isoforms, can be observed from about 1012 weeks of gestation in human fetal quadriceps. Myosin heavy chain isoforms are expressed sequentially during development and are influenced by both innervation and hormones. Primary myotubes are innervated by pioneering axons at an early phase of myogenesis, and most express slow myosin and are destined to become slow, type 1 fibres. It has been proposed that these constitute the fundamental motor units of the developing neuromuscular system and are responsible for early slow movements. Secondary myotubes, however, are hybrid fibres and can express various combinations of fetal/neonatal, fast and slow myosin. These become organized into large, fast motor units later in development, eclipsing the original slow response. In human fetal quadriceps muscles, a population of very small myotubes secondary myotubes, sometimes referred to as tertiary myotubes appears at about 1213 weeks of gestation. At birth, a number of fibres stain histochemically as 2C fibres and coexpress fetal myosin with fast or slow myosin. In our experience, many fibres from neonates express fetal/neonatal myosin; however, by 34 months of age very few may be seen, and a few may remain up to 1 year of age. The embryonic isoform of myosin is not usually detected in neonatal human muscle, except in pathological situations, preterm cases or cases with delayed maturation.
Related Products
Additional information:
Usage: p.r.n.
Tags: buy 75 mg effexor xr with amex, discount 75 mg effexor xr otc, cheap effexor xr 75 mg buy online, generic effexor xr 75 mg with mastercard
Customer Reviews
Real Experiences: Customer Reviews on Effexor XR
Jens, 40 years: This chapter is divided into two major subsections based on this concept: acute immunosuppression and chronic immunosuppression. Histologic features include pigment incontinence with accumulation of melanophages and increased melanin in dermal or epidermal layers.
Kayor, 26 years: The microscopic picture included perineuritis with fibrosis and axonal degeneration. EhlersDanlos syndrome comprises a group of phenotypically similar conditions that frequently result from abnormalities in the structure of collagens or in enzymes modifying collagens molecules.
Brenton, 53 years: Several different skin manifestations can become apparent during the course of onchocerciasis. The mechanism of hypopigmentation in lupus is not known but could be postinflammatory or cicatricial.
Hanson, 23 years: Fourth ventricular tumours are often calcified whereas cystic degeneration is more common in tumours of the lateral ventricles. The glial and mesenchymal elements of gliosarcomas share similar genetic alterations.
Tuwas, 47 years: As of 1991, only 31 cases were described in publications, 21 from autopsy material. Young patients (under 45 years of age) have substantially improved clinical outcomes compared to older counterparts.
Bandaro, 49 years: The ends of the fibrils appear less tightly packed, giving a somewhat frayed appearance. Moreover, it is important to separate anaplastic oligodendrogliomas from malignant small cell astrocytic neoplasms, i.
Kor-Shach, 27 years: Thin cytoplasmic processes often impart a gliofibrillary background, which is variable from area to area. Cutaneous manifestations of disseminated aspergillosis are uncommon, occurring in only 5%10% of patients.
Mazin, 43 years: These features are better appreciated on cytology preparations than in histopathological slides. In longitudinal sections, the abnormal accumulation of filaments is distributed focally along the length of the axon, interposed with more normal axoplasm.