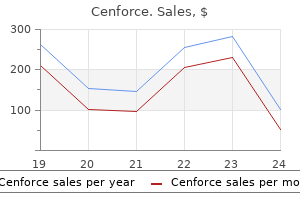
Only $0.56 per item
Cenforce dosages: 200 mg, 150 mg, 130 mg, 100 mg, 50 mg, 25 mg
Cenforce packs: 10 pills, 20 pills, 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
In stock: 863
10 of 10
Votes: 28 votes
Total customer reviews: 28
Description
The distribution of smooth muscle is typical for the intestinal tract treatment h pylori generic 100mg cenforce with amex, with inner circular and outer longitudinal layers of muscle. At the perineal flexure of the rectum, the inner circular layer increases in thickness to form the internal anal sphincter. The internal anal sphincter is under autonomic control (sympathetic and parasympathetic) and is responsible for 85% of resting anal pressure. The outer longitudinal layer of smooth muscle becomes concentrated on the anterior and posterior walls of the rectum, with connections to the perineal body and coccyx, and then passes inferiorly on both sides of the external anal sphincter. The external anal sphincter is composed of striated muscle that is tonically contracted most of the time and can also be voluntarily contracted. Following is a description of an overlapping sphincteroplasty repair for fecal incontinence: 1. The mucosa of the vagina is separated from the anterior wall of the rectum sufficiently laterally and superiorly to provide access to the retracted muscles. Lateral dissection is performed until the ends of the sphincters can be identified. I prefer to divide the scar in the middle, leaving the two ends of the sphincter with the scar attached. It is important to divide the scar but not to trim it from the ends of the sphincter because it will provide tensile strength when the repair is done. The sphincter ends are sufficiently mobilized to allow overlapping of the muscle and are grasped with Allis clamps. If both internal and external muscles are injured, it is preferable to repair them as one unit. This is best performed by incorporating small bites of the anterior wall of the rectum into the sphincteroplasty. Some advocate merely approximating the muscles, but if possible, I prefer to overlap the muscle ends, thus performing an overlapping sphincteroplasty. During the repair, irrigation of the wound is carried out with an antibiotic solution. Also, if necessary, a distal levatorplasty may be performed to decrease the size of the vaginal introitus. At the completion of the repair, the anal canal should be tightened so that it allows just an index finger to be admitted. If the ends of the anal sphincter are significantly refracted, then it becomes impossible to perform an overlapping sphincteroplasty. This is commonly seen when there is complete breakdown of a third- or fourth-degree episiotomy repair. Note that there is complete loss of the perineal body with significant retraction of the external anal sphincter. Sutures are passed through the retracted edges of the external anal sphincter on each side.
Russian Root (Ginseng, Siberian). Cenforce.
- Are there any interactions with medications?
- Common cold. Some research suggests that taking a specific commercial product containing Siberian ginseng plus andrographis (Kan Jang) might reduce some symptoms of the common cold.
- Improving athletic performance.
- How does Ginseng, Siberian work?
- A viral infection called herpes simplex 2.
- Are there safety concerns?
- Dosing considerations for Ginseng, Siberian.
- What other names is Ginseng, Siberian known by?
- What is Ginseng, Siberian?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96946
However medications via endotracheal tube cheap cenforce 150 mg amex, it may be difficult for a child and the parent to comply with frequent suctioning. If aural toilet and topical treatment fail and the microorganisms are not sensitive to oral antibiotics, culture-directed intravenous antibiotics, removal of the tube(s) or, rarely, simple mastoidectomy should be considered. In older children with recurrent episodes of otorrhea, removal of the tube is the treatment of choice, since in these children the eustachian tube may have matured and secretions from the nasopharynx may be refluxing into the middle ear. Also, the tube may occasionally act as a foreign body, causing a foreign body reaction with granulation tissue and infections. If the blockage cannot be resolved 775 but the middle-ear is effusion-free with normal middle-ear pressure, the tube can be left in place and watched until extrusion. If, however, fluid has accumulated in the middle ear or recurrent infections continue, replacement of the tube should be considered. Early Extrusion Premature extrusion of tympanostomy tubes occurs in approximately 3. Displacement of Tympanostomy Tube into the Middle-Ear the incidence of displacement of a tympanostomy tube into the middle-ear is 0. If the tube is displaced into the middle ear during surgery attempts should be made to retrieve the tube at the time of surgery. Indications for removing a tympanostomy tube include: one tube is retained while the other tube has extruded and the middle ear has been free of disease for one year or longer in a child five to six years or older; bilateral retained tubes in an older child with good eustachian-tube function; chronic or recurrent episodes of otorrhea that are not able to be managed 776 medically, especially in an older child who previously has not had recurrent episodes of otorrhea, as this could be a sign of reflux of secretions from the nasopharynx due to maturation of the eustachian tube; and the tympanostomy tube is imbedded in granulation tissue and the tube is blocked. After the tube has been removed, a paper patch or gelfoam myringoplasty is performed. Soft long-term T-tubes may be removed in the office in older, cooperative children. These children must be followed to see if the perforation closes spontaneously or a myringoplasty is required. Water Precautions Several studies have been published, including two meta-analyses229,230 demonstrating no increase in episodes of otorrhea in patients with tympanostomy tubes not using water precautions compared to those using water precautions. In a clinical trial to assess the need for water precautions for children with tympanostomy tubes, Goldstein et al. However, the clinical impact of using ear plugs for most children was small and their use should be individualized rather than recommended on a routine basis. The prevalence of tympanic-membrane retractions decreased over time, whereas myringosclerosis remained unchanged in M&T ears and increased in M ears. The extension of myringosclerosis increased whereas extension of atrophy and pars tensa retraction decreased over time regardless of treatment 777 modality.
Specifications/Details
A gallium-67 scan treatment uterine fibroids buy cenforce 150mg overnight delivery, showing areas of active infection, will have increased uptake early in the disease and will clear as the infection is controlled. Both the technecium-99 bone scan and the gallium67 scan are ordered initially; the technecium bone scan confirming the diagnosis by demonstrating bone involvement; and the gallium scan to confirm the infectious process. The erythrocyte sedimentation rate can also be monitored to assess the resolution of infection. Before the availability of the quinolones, this usually meant an aminoglycoside (such as gentamicin) in combination with an antipseudomonal penicillin (such as piperacillin) or a third-generation cephalosporin. These treatments could only be given intravenously, and a sixweek course was usually required. This usually meant a prolonged hospital stay and some degree of vestibular impairment due to the aminoglycoside. The quinolones, such as ciprofloxacin, provided excellent pseudomonal coverage in the oral form, allowing most patients with necrotizing otitis externa to be treated on an outpatient basis. This antibiotic regimen may be altered based on the results of the culture and the effectiveness of the therapy, as determined by a gallium scan six weeks after starting therapy. Results of this intervention were often disappointing as it often facilitated the spread of the disease. Currently, surgical intervention is avoided as it may promote the spread of infection and is only used after failure of prolonged antibiotic therapy. Unlike bacterial infections, pain seems to be an uncommon complaint in these infections, whereas the usual complaint is puritus. Much of the time, fungus found in the ear canal is saprophytic, meaning that it grows on dead organic matter. This most often occurs in cases of chronic suppurative otitis media where the pus serves as a food source for the fungus. In 692 such cases, the fungus involved, usually aspergilllus, is not a true infective pathogen. Debridement of granulation and necrotic tissue and treatment of the underlying suppuration will usually resolve the fungal overgrowth. Saporophytes, however, can become invasive infectious microorganisms when there is significant immune suppression or limited circulation of blood. Invasive fungal infections can be rapidly fatal and requires aggressive treatment. The fungal hyphae often spread in the endothelial layer of the blood vessels, causing hypoperfusion and necrosis (as seen in mucormycosis). Aggressive surgical debridement, correction of immune suppression and high-dose amphotericin B are appropriate therapy for these frail patients. Another common fungal infection found in the external ear is due to Candida species. Patients may complain of pruritus, a smelly discharge from the ear and a hearing loss due to the accumulated debris.
Syndromes
- Chronic active hepatitis
- Developmental delay
- The person has a history of severe allergic reactions (check for a medical ID tag).
- Various colognes
- Heart valve lesions
- Breathing problems
- Arterial blood gases
- Tests to look for early cancer
Dynamic endoscopic inspection of the eustachian-tube orifice is important in differentiating whether the cause of dysfunction may be a mucosal or obstructive problem versus a muscular dilatory failure treatment 3rd degree heart block cheap cenforce 25mg. Tubal dysfunction is then classified as either an obstructive or dynamic disorder. To evaluate normal dilation, the patient is then instructed to do a series of swallows. To evaluate maximal dilatory effort, the patient is then instructed to do a series of yawns. The tube should be seen going from the closed S position into a rounded open lumen and relax back to its resting closed state. Slow-motion video endoscopy is also used to evaluate eustachian-tube opening further, particularly in patients with chronic tubal dysfunction. Images captured on video are reviewed in slow motion to evaluate the eustachian-tube dynamics in detail. Each of the four phases of Eustachian-tube opening along with the dynamic function of both the tensor veli palatini and levator veli palatini can be isolated and evaluated using this technique. Eustachian-Tube Function Tests 717 A number of tests have been employed using either positive or negative pressure through the external auditory canal or nasopharynx to assess eustachian-tube function. Unfortunately, none of these tests have gained widespread use as they all lack clinical significance. The forced response test measures the pressure needed to open the eustachian tube and requires a patent ventilation tube or perforation. The external auditory canal is then sealed; and, using a tympanometry probe, the pressure is increased until the eustachian tube opens resulting in a sudden decompression. The inflation-deflation test developed by Bluestone is a nine-step tympanometric evaluation during ear-canal inflation and deflation. The first step is a traditional tympanogram assessing the baseline middle-ear pressure. The second step involves placing positive pressure within the ear canal and instructing the patient to equalize this pressure by opening the eustachian tube typically by swallowing. The third step removes the positive pressure within the ear canal leaving a slight negative pressure within the middle-ear space. In the fourth step, the patient once again tries to equalize the middle-ear pressure by swallowing. The fifth step then allows air to flow from the nasopharynx into the middle ear with the acquisition of a tympanogram. The sixth step then applies a negative pressure to the external auditory canal and the patient tries to equalize the pressure by opening the eustachian tube. The seventh step involves removing the negative pressure from the ear canal, which results in a slight positive pressure within the middle-ear cavity. The patient then attempts to equalize this slight positive pressure and a tympanogram is obtained (Steps 8 and 9).
Related Products
Additional information:
Usage: q._h.
Tags: 100mg cenforce order with visa, generic cenforce 25mg online, purchase cenforce 25 mg otc, 130mg cenforce with amex
Customer Reviews
Real Experiences: Customer Reviews on Cenforce
Quadir, 30 years: Peripheral Auditory System A traditional approach toward understanding the primary sensitivity, frequency tuning, and timing functions of the peripheral auditory system is to divide it into 3 discrete parts.
Kadok, 53 years: As their name implies, the generic measures are generalizable across health conditions, practice settings, and types of treatments.
Torn, 60 years: Hearing aids and other devices are evaluated to verify proper functioning when they are received from the manufacturer and before they are dispensed to a patient.
Mason, 22 years: A thorough family history is important, including the age of onset, severity and rate of progression of any hearing loss.
Stejnar, 38 years: After the vaginal dissection has been completed, a long curved clamp is passed medially into the vaginal incision, thus creating a tunnel that the fat pad will pass through to reach the vaginal area.
Will, 49 years: The advantages and disadvantages of these three approaches have been summarized in Table 35-8.
Rendell, 33 years: Minimally invasive drug delivery to the cochlea through application of nanoparticles to the round window membrane.