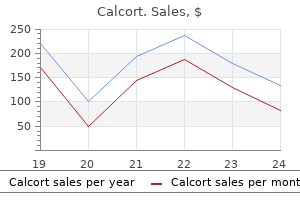
Only $1.51 per item
Calcort dosages: 6 mg
Calcort packs: 30 pills, 60 pills, 120 pills, 240 pills, 300 pills
In stock: 624
8 of 10
Votes: 181 votes
Total customer reviews: 181
Description
With moderate to severe regurgitation medications vertigo generic calcort 6mg buy on line, tricuspid annuloplasty may be performed in conjunction with replacement of another valve. Recent studies suggest that correction of significant tricuspid regurgitation is beneficial when patients are brought to surgery for replacement of another valve. The risk of antibiotic administration is often considered greater than the potential for developing perioperative endocarditis. Such conditions include: · Patients with prosthetic cardiac valves or prosthetic heart materials · Patients with a past history of endocarditis Anesthetic Management A. Objectives Hemodynamic goals should be directed primarily toward the underlying disorder. Positive end-expiratory pressure and high mean airway pressures may also be undesirable during mechanical ventilation because they reduce venous return and increase right ventricular afterload. Pulmonary artery catheterization is not always possible; rarely a large regurgitant flow may make passage of a pulmonary artery catheter across the tricuspid valve difficult. Thermodilution cardiac output measurements are falsely elevated because of the tricuspid regurgitation. Choice of Agents the selection of anesthetic agents should be based on the underlying disorder. Reasonable Endocarditis prophylaxis is reasonable for patients with the highest risk of adverse outcomes who undergo dental procedures that involve manipulation of either gingival tissue or the periapical region of teeth or perforation of the oral mucosa. Endocarditis is believed to occur in areas of cardiac endothelial damage, where in cases of bacteremia, bacteria can be deposited and multiply. Areas of increased myocardial blood flow velocity lead to damaged endothelium, providing a template for bacterial adherence and growth. Moreover, they note that although prophylaxis is not suggested for respiratory tract procedures, it is a reasonable strategy in high-risk patients in whom an incision has been made in the respiratory tract (eg, in tonsillectomy). Guidelines are ever changing, and although not considered to be "standard of care," they are increasingly present in medical practice; furthermore, deviation from guidelines often requires explanation as being outside of "evidenced-based" practice. Aspirin is also indicated in this population, as well as in patients with bioprosthetic valves, to prevent thrombus formation. Warfarin is sometimes also used initially for mitral bioprosthetic valves (Table 2116). Patients with prosthetic valves often present for noncardiac surgery that will require temporary discontinuation of anticoagulation. In patients receiving warfarin, aspirin is recommended in virtually all situations. Heparin can be discontinued 46 hours prior to surgery and then restarted as soon as surgical bleeding permits, until the patient can be restarted on warfarin therapy. Fresh frozen plasma may be given, if needed, in an emergency situation to interrupt warfarin therapy.
Lu-Hui (Aloe). Calcort.
- Is Aloe effective?
- Psoriasis.
- What is Aloe?
- Dosing considerations for Aloe.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96602
Extubation may be considered for older treatment for depression calcort 6 mg order with visa, relatively healthy patients undergoing simple procedures such as closure of a patent ductus or atrial septal defect or repair of coarctation of the aorta. Cardiac Transplantation Preoperative Considerations Cardiac transplantation is the treatment of choice for otherwise healthy patients with end-stage heart disease so severe that they are unlikely to survive the next 612 months. The procedure is generally associated with 8090% postoperative survival at 1 year and 6090% survival at 5 years. Transplantation improves the quality of life and most patients are able to resume a relatively normal lifestyle. Unfortunately, the number of cardiac transplants performed is limited by the supply of donor hearts, which are obtained from brain-dead patients, most commonly following intracranial hemorrhage or head trauma. Intractable heart failure may be the result of a severe congenital lesion, ischemic cardiomyopathy, viral cardiomyopathy, peripartum cardiomyopathy, a failed prior transplantation, or valvular heart disease. Medical therapy should include the standard drugs used for heart failure, including angiotensin-converting enzyme inhibitors (or angiotensin receptor blockers, or both) and blockade (usually with carvedilol). Other drugs may include diuretics, vasodilators, and even oral inotropes; oral anticoagulation with warfarin may also be necessary. Patients may not be able to survive without intravenous inotropes while awaiting transplantation. Transplant candidates must not have suffered extensive end-organ damage or have other major systemic illnesses. Reversible renal and hepatic dysfunction are common because of chronic hypoperfusion and venous congestion. Patients with long-standing pulmonary hypertension may, however, be candidates for combined heartlung transplantation. Premature induction of anesthesia unnecessarily prolongs the time under anesthesia for the recipient, whereas delayed induction may jeopardize graft function by prolonging the period of ischemia. Patients may receive little advance warning of the availability of a suitable organ. Many-if not most-will have eaten a recent meal and should be considered to have a full stomach. Administration of a clear antacid (sodium citrate), a histamine H2receptor blocker, and metoclopramide should be considered. Any sedating premedication may be administered intravenously just prior to induction. Monitoring is similar to that used for other cardiac procedures and is often established prior to induction. Use of the right internal jugular vein for central access does not appear to compromise its future use for postoperative endomyocardial biopsies. Induction may be carried out with small doses of opioids (fentanyl, 510 mcg/kg) with or without etomidate (0. Aminocaproic acid or tranexamic acid can be used to decrease postoperative bleeding. If a pulmonary artery catheter was placed, it must be completely withdrawn from the heart with its tip in the superior vena cava.
Specifications/Details
A surprisingly large fraction of patients undergoing elective surgery will be receiving one of these agents treatment 1st degree burns buy calcort 6 mg without a prescription. These agents have little or no anticholinergic activity and do not generally affect cardiac conduction. Lithium dilution cardiac output measurements are contraindicated in patients on lithium therapy. This disorder is thought to be related to an excess of dopaminergic activity in the brain. The most commonly used antipsychotics include phenothiazines, thioxanthenes, phenylbutylpiperadines, dihydroindolones, dibenzapines, benzisoxazoles, and butyrophenones. Older antipsychotic medications had strong dopamine antagonistic effects, leading to extrapyramidal side effects (eg, muscle rigidity and progression to tardive dyskinesia). Other agents have less dopamine antagonism and occupy the D2 dopamine receptor to a lesser degree, thereby reducing extrapyramidal effects. The antipsychotic effect of these agents seems to be due to dopamine antagonist activity. Side effects include orthostatic hypotension, acute dystonic reactions, and parkinsonism-like manifestations. Risperidone and clozapine have little extrapyramidal activity, but the latter is associated with a significant incidence of granulocytopenia. Reduced anesthetic requirements may be observed in some patients, and some patients may experience perioperative hypotension. In its most severe form, the presentation is similar to that of malignant hyperthermia. Muscle rigidity, hyperthermia, rhabdomyolysis, autonomic instability, and altered consciousness are seen. Treatment with dantrolene seems to be effective; bromocriptine, a dopamine agonist, may also be effective. Characteristically, with chronic abuse, patients develop tolerance to the drug and varying degrees of psychological and physical dependence. Physical dependence is most often seen with opioids, barbiturates, alcohol, and benzodiazepines. Lifethreatening complications primarily due to sympathetic overactivity can develop during abstention. The history of substance abuse may be volunteered by the patient (usually only on direct questioning) or deliberately hidden. Anesthetic requirements for substance abusers vary, depending on whether the drug exposure is acute or chronic (see Table 284). Elective procedures should be postponed for acutely intoxicated patients and those with signs of withdrawal. When surgery is deemed necessary in patients with physical dependence, perioperative doses of the abused substance should be provided, or specific agents should be given to prevent withdrawal. Multimodal approaches to pain control are useful perioperatively, and patients should be started on maintenance methadone as soon as possible.
Syndromes
- An experimental treatment called corneal cross-linking causes the cornea to become hard and stops the condition from getting worse. The cornea can then be reshaped with laser vision correction.
- Pancreatic venous sampling for insulin
- Endotracheal intubation to prevent the windpipe from swelling shut due to burns
- Breathing tube
- Dizziness
- The name of the product (ingredients and strengths, if known)
- Name of product (as well as the ingredients and strength, if known)
- Psychometric testing
- Stool culture may be positive for a certain type of E. coli bacteria or other bacteria
In contrast symptoms stomach flu cheap calcort 6mg otc, inadequate insertion depth will position the cuff in the larynx, predisposing the patient to laryngeal trauma. Inadequate depth of insertion can be detected by palpating the cuff over the thyroid cartilage. Mediastinitis presents as severe sore throat, fever, sepsis, and subcutaneous air often manifesting as crepitus. If esophageal perforation is suspected, consultation with an otolaryngologist or thoracic surgeon is recommended. Even though it is confirmed that the tube is in the trachea, it may not be correctly positioned. Hemodynamic changes can be attenuated by intravenous administration of lidocaine, opioids, or -blockers or deeper planes of inhalation anesthesia in the minutes before laryngoscopy. Hypotensive agents, including sodium nitroprusside, nitroglycerin, esmolol and nicardipine, have also been shown to effectively attenuate the transient hypertensive response associated with laryngoscopy and intubation. Cardiac arrhythmias-particularly ventricular bigeminy-sometimes occur during intubation and may indicate light anesthesia. Laryngospasm is a forceful involuntary spasm of the laryngeal musculature caused by sensory stimulation of the superior laryngeal nerve. Laryngospasm is usually prevented by extubating patients either deeply asleep or fully awake, but it can occur-albeit rarely-in an awake patient. Treatment of laryngospasm includes providing gentle positive-pressure ventilation with an anesthesia bag and mask using 100% oxygen or administering intravenous lidocaine (11. The large negative intrathoracic pressures generated by a struggling patient during laryngospasm can result in the development of negative-pressure pulmonary edema, even in healthy patients. Whereas laryngospasm may result from an abnormally sensitive reflex, aspiration can result from depression of laryngeal reflexes following prolonged intubation and general anesthesia. Bronchospasm is another reflex response to intubation and is most common in asthmatic patients. Other pathophysiological effects of intubation include increased intracranial and intraocular pressures. Polyvinyl chloride tubes may be ignited by cautery or laser in an oxygen/nitrous oxide-enriched environment. What are some important anesthetic considerations during the preoperative evaluation of a patient with an abnormal airway Induction of general anesthesia followed by direct laryngoscopy and oral intubation is dangerous, if not impossible, in several situations. Any available prior anesthesia records should be reviewed for previous problems in airway management. If a facial deformity is severe enough to preclude a good mask seal, positive-pressure ventilation may be impossible. These two groups of patients should generally not be allowed to become apneic-including induction of anesthesia, sedation, or muscle paralysis-until their airway is secured.
Related Products
Additional information:
Usage: p.o.
Tags: 6 mg calcort buy overnight delivery, cheap calcort 6mg buy on-line, calcort 6 mg buy fast delivery, 6mg calcort otc
Customer Reviews
Kurt, 53 years: The outcome from a head injury is dependent not only on the extent of the neuronal damage at the time of injury, but also on the occurrence of any secondary insults. Immediate postoperative extubation may be considered if the patient is comfortable, cooperative, physiologically stable, and not hemorrhaging significantly.
Rufus, 46 years: This may result from obstruction, altered motility, or abnormal sphincter function. If neither of these end points is achieved, the patient should remain intubated and ventilation should be continued.
Stejnar, 57 years: Death from an unexpected circulatory arrest, usually due to a cardiac arrhythmia occurring within an hour of the onset of symptoms, in whom medical intervention. These techniques have never been popular in North America due to concerns about the risk of spinal hematomas following heparinization, the associated medicallegal consequences, and the limited evidence of an outcome benefit.
Rozhov, 32 years: The relative contribution of these parameters has been tuned to correlate with the degree of sedation produced by various sedative agents. As soon as the double-lumen tube is placed, both bronchial and tracheal cuffs should be inflated.